📌 Key Takeaways
The first week on a new sleep prescription works best when you time the dose around tomorrow’s alarm, not tonight’s bedtime.
- Start From Wake Time: Count backward from when you need to be alert — that math gives you the right dosing window.
- Protect a Full Sleep Block: Skipping a dose beats taking one with only four or five hours before your alarm.
- Give It a Week, Not One Night: Most bodies need 3–7 nights to adjust, so one groggy morning doesn’t mean the medication failed.
- Shift Timing Before Changing Dose: Moving the dose 30–60 minutes earlier fixes most morning grogginess — dose changes need your doctor.
- Track Mornings, Not Feelings: A simple daily log of dose time, sleep hours, and a 1–10 clarity score reveals patterns guessing never will.
One rough morning is a data point, not a verdict — seven nights of consistent timing tell the real story.
Shift workers and busy professionals starting a non-controlled sleep prescription will find a clear first-week game plan here, preparing them for the detailed adjustment guide that follows.
~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~
Medically reviewed by David Danish, MD, and Peter Kelly, DO
The alarm screams. Your eyelids weigh ten pounds each.
You’re gripping the bathroom counter, trying to decide whether you can safely drive to the hospital, the warehouse, the plant. The medication was supposed to help. Was last night a mistake?
That fear — one groggy morning proving the whole prescription was wrong — stops more shift workers from finding real sleep than any side effect ever could. You picked up a non-controlled sleep aid because nothing else worked. Melatonin was useless. Over-the-counter antihistamines turned you into a zombie by hour three of your shift.
Here’s what most people miss: the medication probably isn’t the problem. The timing is. Non-controlled sleep aids like hydroxyzine, clonidine, and trazodone are well-tolerated, routine prescriptions that millions of people use safely. They work as sleep facilitators, not chemical knockouts — helping the body settle into sleep rather than forcing unconsciousness. Timing relative to when you need to be fully alert is the single biggest lever you control during your first week.
“I’ve tried a bunch of different things for my sleep, and most of them either didn’t work or made me feel like a zombie the next day. Haven’t slept this well in years.” — Jessica
Start with Tomorrow’s Alarm, Not Tonight’s Bedtime
The most useful first-week question isn’t “What time should I take this?” It’s: What time do I need to be completely functional tomorrow?
Work backward from that answer. If your shift starts at 6:00 AM and you need 45 minutes to get ready, you need to be clear-headed by 5:15 AM. Count back 7–8 hours for a protected sleep block, then subtract an additional 30–60 minutes to account for the medication’s onset time. That backward math gives you a concrete dosing window — not a vague “take at bedtime.”
One critical rule: if you only have four or five hours before your next alarm, skip the dose. These medications need a full sleep window for their strongest sedative effects to wear off, even though they can remain in your system much longer. Taking them with a short window is one of the most common causes of next-morning grogginess.
This principle works whether you’re on a fixed schedule, a rotating shift, or somewhere in between. Start with wake time, not with when the shift ends.
Your First 7 Nights: The Adjustment Rules That Matter Most
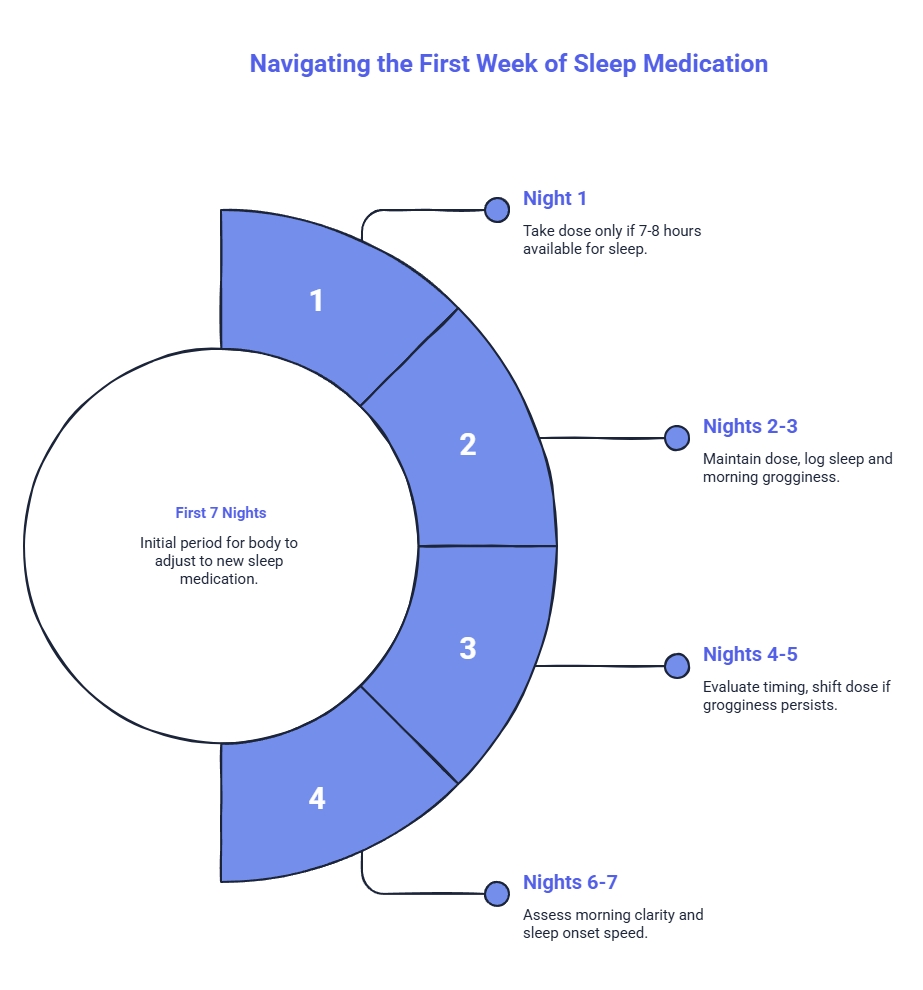
Your body typically needs 3 to 7 days to adapt to a new non-controlled sleep prescription. Think of the first week as observation, not judgment. One rough morning does not mean the medication failed.
Night 1 — Protect the full window. Take your prescribed dose only when you genuinely have 7–8 hours before you need to be alert. If tonight isn’t that night, wait. “Dosing” here means using the prescribed amount exactly as directed — not experimenting with a different quantity.
Nights 2–3 — Hold steady and observe. Keep your dose exactly as prescribed. Don’t change the timing yet. Log when you fell asleep, when you woke up, and how your head felt 30 minutes after waking. Early grogginess can happen during the adjustment period, and that alone does not prove failure.
Nights 4–5 — Evaluate timing, not the dose. If mild grogginess lingers, ask whether you’re taking the medication too close to wake time. Shifting the dose 30–60 minutes earlier — while still protecting that full sleep block — resolves the issue for many people. Any change to the actual dose amount is a conversation with your provider, not a solo decision.
Nights 6–7 — Look for the trend. Are mornings getting clearer? Is sleep onset getting faster? If the answer is yes, you’re adjusting normally. If grogginess hasn’t budged despite good timing and a full sleep window, contact your provider for a medication or dose review.
What These Numbers Look Like in Practice
Every patient’s prescription is individualized, but a few reference points help set expectations during week one.
Hydroxyzine is commonly prescribed at 25–50 mg, taken 30–60 minutes before bedtime. Sedation typically begins within 15–30 minutes. While it can support a 4–8 hour sleep window, its long half-life means drowsiness may persist into the next morning. It tends to work well when insomnia is driven by racing thoughts or anxiety at bedtime.
Clonidine typically starts at 0.1 mg, also taken 30–60 minutes before bed. Physicians often follow a low-and-slow approach, and the same best-practice rule applies: take it only when you’re ready for a full 7–8 hour sleep block.
Trazodone is another non-controlled option SleepScriptMD prescribes for sleep maintenance, though dosing and timing are tailored to each patient’s profile during their physician review.
For a broader overview of how these options fit different sleep patterns, read the guide to non-habit-forming sleep meds. For timing windows specific to each medication, that resource walks through hydroxyzine, clonidine, trazodone, and other options in detail.
What to Track Each Morning So You Stop Guessing
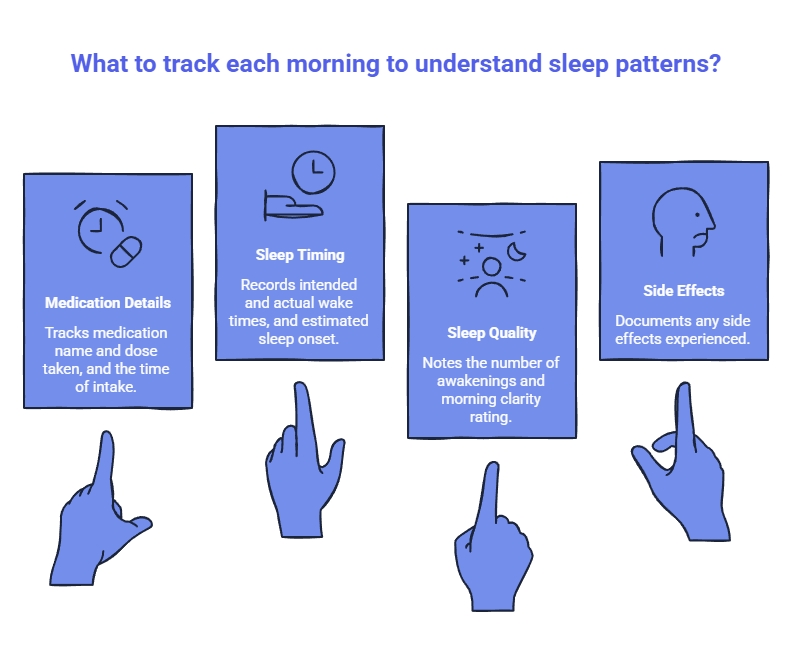
The difference between “this doesn’t work” and “I need to shift my timing by 30 minutes” often lives in data you forgot to capture. Each morning, jot down:
- Medication name and prescribed dose taken
- Clock time you took the dose
- Intended wake time
- Estimated time you fell asleep
- Number of awakenings
- Actual wake time
- Morning clarity rating on a 1–10 scale (heavy / okay / clear-headed)
- Any side effects like dry mouth or mild dizziness
Seven mornings of this log gives you and your physician a picture no single morning can provide. Keep it on your nightstand or your phone — somewhere you’ll reach before the coffee kicks in and the details blur.
The point isn’t to build a perfect spreadsheet. The point is to notice patterns. Maybe the worst mornings follow a late dose. Maybe grogginess is tied to a shortened sleep block. Maybe timing improves after a small shift earlier, while the prescribed amount stays exactly the same.
The Common Mistakes That Cause Preventable Grogginess
Morning fog isn’t always about the drug itself. Often, it’s about what happened around it — and most early problems are logistical rather than dramatic.
Failing to protect the full metabolic window is the primary driver of residual morning sedation. If your body needs 7–8 hours to metabolize the dose and you gave it 5, you’ll feel the difference. Taking it without a real sleep window — hoping four hours is enough — often leads to residual sedation the next morning.
Avoid alcohol entirely while taking these medications, as combining them can dangerously amplify sedation and cause severe respiratory side effects. Caffeine consumed after early afternoon can compress your effective sleep window. Screens or mental stimulation after taking the dose work against a medication designed to facilitate sleep rather than force it. And taking the medication only to continue working, scrolling, or staying mentally switched on works against what the prescription is designed to do.
None of these are character flaws. They’re logistical problems with straightforward fixes. A calmer pre-sleep routine can make the prescription work noticeably better, especially when shift work already pushes the body out of its natural rhythm. For general background on how reversed schedules affect sleep biology, the NHLBI overview on shift work and sleep is a useful starting point.
What Is Normal in Week One vs. When to Contact Your Provider
Most early side effects resolve on their own within the first few days. Common during the first 3–7 days: mild morning grogginess that improves as the week progresses, dry mouth, mild dizziness when standing quickly, and sleep that’s better but “not perfect yet.” These are adjustment signals, not alarms.
Contact your provider if: grogginess persists despite protecting a full sleep block and optimizing timing, side effects interfere with safe job performance, you have concerns about medication interactions or a change in health status, or the issue clearly isn’t timing and you need a dose review.
If you’re already a SleepScriptMD patient, you can report side effects or request a dose adjustment through the Returning Patient Portal — the same asynchronous care model you used for your initial prescription. No waiting room, no phone call.
When This Article Does Not Apply
This guide is for eligible, low-risk adults using non-controlled sleep prescriptions for the first time. SleepScriptMD treats patients who meet specific safety criteria and routes everyone else to appropriate in-person care.
You’ll need in-person evaluation if you fall outside the eligible age range, are pregnant or planning to become pregnant, have a major medical condition or active substance use disorder, or suspect something beyond standard insomnia. Sudden daytime sleep attacks, physically acting out dreams, or an uncontrollable urge to move your legs at night each require specialized testing. If you’ve been told you snore heavily or stop breathing during sleep, an at-home sleep test is required before any medication review continues.
Your Week-One Checkpoint
That first week wasn’t your baseline—it was just the system settling into place? That was one data point, not a verdict.
The first week should feel like a plan, not a gamble. Work backward from wake time. Protect a real sleep block. Keep the prescribed dose stable. Track what happens. Give the body a few nights to settle. Seven nights of consistent timing and a simple morning log will tell you more than a hundred nights of guessing. The goal isn’t a perfect night one. It’s a trend line moving in the right direction by night seven.
Clear mornings are closer than one rough night makes them feel.
If you haven’t started treatment yet and you’re ready for a physician-led evaluation built for unpredictable schedules, start your secure intake from your phone — no appointment, no waiting room, no video call.
Disclaimer: This article is for educational purposes only and does not replace personalized medical advice. Start, stop, or change prescription sleep medication only under clinician guidance. If you experience severe side effects, worsening symptoms, or a medical or mental health emergency, seek urgent in-person care immediately.
Our Editorial Process:
Our expert team uses AI tools to help organize and structure our initial drafts. Every piece is then extensively rewritten, fact-checked, and enriched with first-hand insights and experiences by expert humans on our Insights Team to ensure accuracy and clarity.
About the SleepScriptMD Insights Team:
The SleepScriptMD Insights Team is our dedicated engine for synthesizing complex topics into clear, helpful guides. While our content is thoroughly reviewed for clarity and accuracy, it is for informational purposes and should not replace professional advice.