📌 Key Takeaways
Non-habit-forming sleep medications work differently than Ambien or Xanax—they help you sleep without creating the same addiction risks.
- Different Brain Pathways Matter: Trazodone, hydroxyzine, and clonidine don’t trigger the reward centers that make controlled sedatives addictive—they calm your system through safer mechanisms.
- OTC Isn’t Always Safer: Benadryl’s 8+ hour grogginess wrecks shift workers more than prescription options designed for flexible dosing and timing.
- Match the Med to Your Pattern: Racing thoughts? Hydroxyzine calms them. Wired but exhausted? Clonidine dials down your nervous system. Waking repeatedly? Trazodone supports deeper sleep.
- Online Care Works for Shift Workers: Complete intake at 3 AM after your shift—a real doctor reviews it during business hours and sends prescriptions to your pharmacy.
- Grogginess Is Fixable: Morning fog usually improves when you adjust timing—take your medication 15–30 minutes earlier relative to your wake-up time.
Sleep meds without addiction risk exist—finding the right fit just takes clinical guidance.
Shift workers, nurses, and anyone whose schedule makes sleep nearly impossible will find practical options here, preparing them for the detailed medication comparisons that follow.
~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~
3:47 AM. The blackout curtains are drawn tight, but your brain didn’t get the memo that it’s supposed to be nighttime. You just finished a 12-hour shift, your body is exhausted, and yet here you are—staring at the ceiling, watching the minutes tick by until your next alarm.
You’ve tried the OTC route. Melatonin did nothing. Benadryl knocked you out but left you feeling like a zombie for your next shift. And the thought of asking for “real” sleep medication? That feels like stepping onto a slippery slope toward dependency, foggy mornings, or both.
Here’s what most people don’t realize: there’s an entire category of prescription sleep support that doesn’t work like Ambien or Xanax. These are non-habit-forming sleep meds—medications that help your body wind down without the severe dependency profile of controlled substances, generally aiming to minimize the intense next-day impairment that keeps shift workers struggling to function.
This guide explains what these medications actually are, how they differ from the options you’ve probably already tried or feared, and how to figure out whether they might be worth exploring for your situation.
The Fast Answer: What “Non-Habit-Forming Sleep Meds” Actually Means
Non-addictive sleep medications are prescription options that don’t carry the same addiction risk as controlled substances like benzodiazepines (Xanax, Ativan) or Z-drugs (Ambien, Lunesta).
Think of them as gentle sleep facilitators rather than chemical knockouts. They work with your body’s existing systems—calming anxiety, quieting an overactive nervous system, or supporting deeper sleep architecture—without hijacking your brain’s reward pathways in ways that create cravings or severe chemical dependency.
The technical distinction matters: these medications are “non-controlled,” meaning they’re not classified by the DEA as having high abuse potential. That’s a significant difference from controlled sedatives, which require stricter prescribing rules precisely because dependency is a known risk.
Non-controlled doesn’t mean side-effect-free. Every medication has potential effects, and what works well for one person may not be the right fit for another. The point isn’t that these options are perfect—it’s that they occupy a different safety category than the medications many people picture when they hear “prescription sleep help.”
Adults dealing with schedule-driven insomnia who want to understand their options beyond OTC products and controlled sedatives. If you work rotating shifts, night shifts, or irregular schedules that make consistent sleep nearly impossible, this information is especially relevant. If you’re reading this in March, daylight-saving changes can make an already fragile shift-work sleep pattern feel even worse—that doesn’t change the big picture, but it explains why some weeks feel dramatically harder than others.
If you’re looking for controlled sedatives specifically, or if you have symptoms suggesting a more complex sleep disorder (we’ll cover those briefly later), this particular care pathway isn’t the right fit. That’s not a judgment—it’s just about matching the right solution to the right problem.
Myth vs. Reality: Why These Meds Are Different From Ambien, Xanax, and OTC Sleep Aids
Most of the fear around prescription sleep medication comes from conflating very different categories.
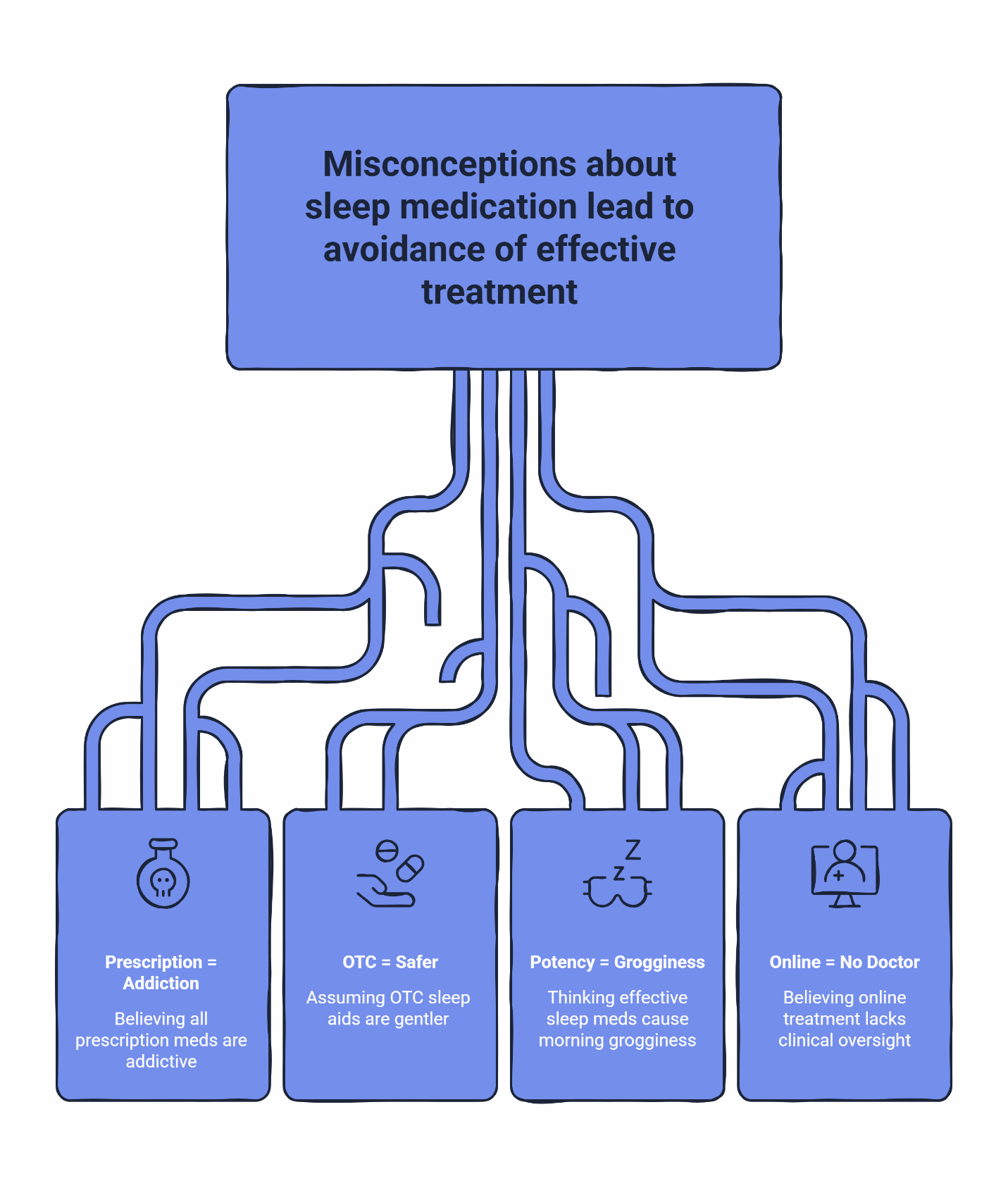
Myth: If it’s prescription-strength, it must be addictive.
Reality: Addiction risk depends on how a medication works in your brain, not just its strength. Controlled sedatives like benzodiazepines and Z-drugs affect GABA receptors in ways that can create physical dependence over time. Non-controlled options like trazodone, hydroxyzine, and clonidine work through entirely different mechanisms—antihistamine effects, serotonin modulation, or nervous system calming—that don’t trigger the same dependency pathways.
Myth: OTC sleep aids are safer because they’re over the counter.
Reality: “Available without a prescription” doesn’t mean “gentler on your system.” Diphenhydramine (Benadryl, ZzzQuil) is an antihistamine that can leave you groggy for 8+ hours—a real problem when your sleep window is only 5-6 hours between shifts. Melatonin may help with jet lag but often isn’t strong enough to override the powerful circadian alerting signals your body sends during daytime sleep attempts. Meanwhile, non-controlled prescription options can be specifically chosen and dosed based on your actual sleep pattern. There’s a reason many shift workers find that OTC sleep aids leave them feeling like zombies—these products weren’t designed with irregular schedules in mind.
Myth: Anything strong enough to actually work will destroy your morning.
Reality: Morning grogginess is about fit, not just potency. The right medication at the right dose, taken at the right time relative to your wake-up, can help you sleep without wrecking your alertness. Some options have shorter half-lives than others. Some people do better with one medication versus another. The key is clinical guidance on timing and dosing—not avoiding prescription help altogether.
Myth: Online sleep treatment means no real doctor is involved.
Reality: Legitimate telehealth platforms use licensed physicians who review your medical history, assess your eligibility, and make individualized treatment decisions. AI tools may help organize intake information or streamline workflows, but a real clinician reviews and approves every prescription. The convenience of digital access doesn’t mean the clinical oversight disappears—it means you can get that oversight without taking time off work for a 3-week-out appointment.
The 3 Main Options People Usually Hear About
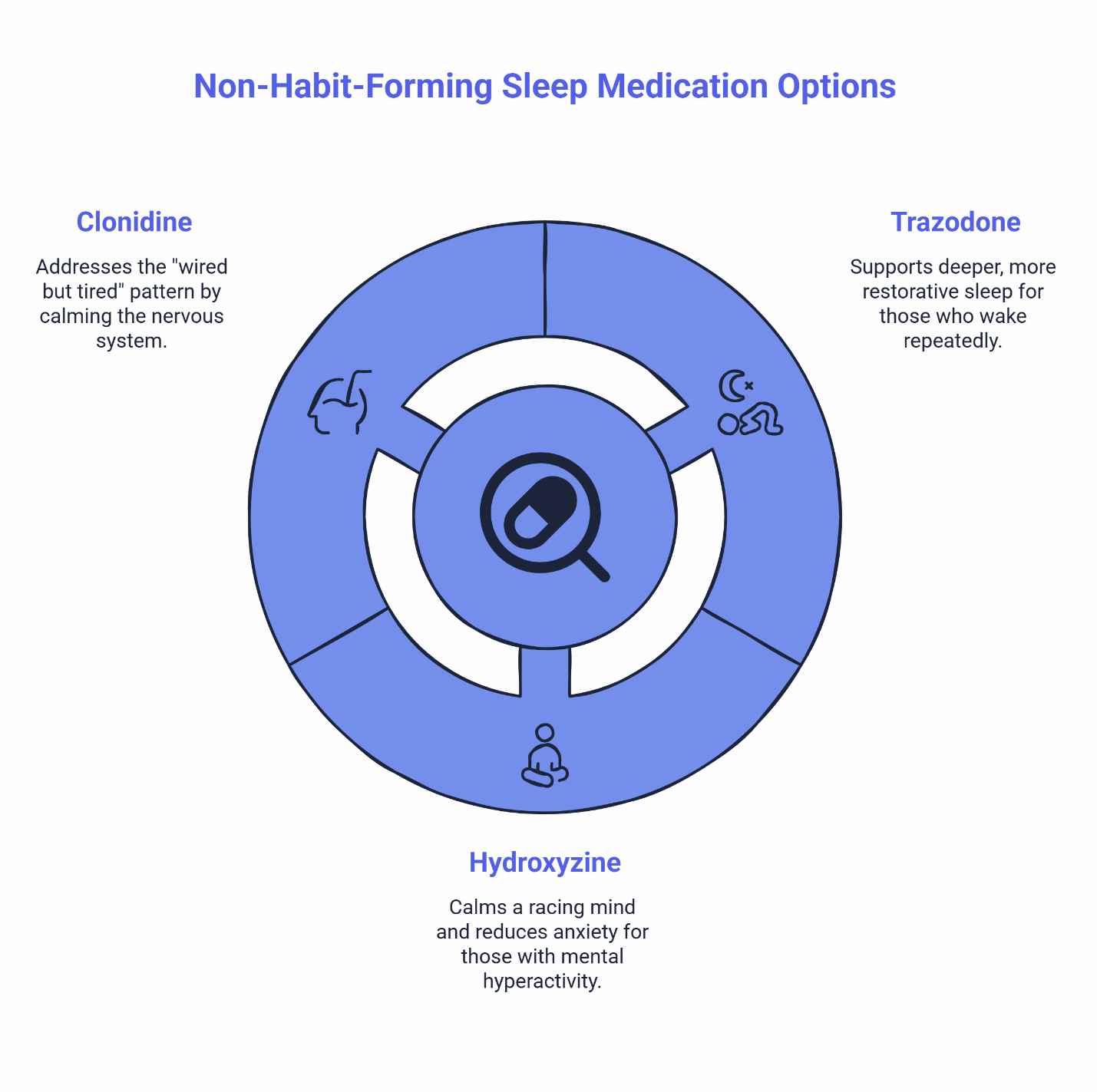
When people start researching non-habit-forming sleep medications, three names come up repeatedly: trazodone, hydroxyzine, and clonidine. Each works differently, and each tends to fit different sleep patterns better than others.
This isn’t a “pick your medication” guide—that’s what clinician review is for. But understanding the general landscape helps you have a more informed conversation about what might make sense for your situation.
Trazodone
What it is: Originally developed as an antidepressant, trazodone is now widely prescribed at lower doses for sleep. It works partly through serotonin pathways and partly through histamine blocking.
What kind of sleep problem it’s commonly discussed for: People who fall asleep okay but wake up repeatedly through the night, or who feel like their sleep is shallow and unrefreshing. Trazodone is often associated with supporting deeper, more restorative sleep.
What people tend to appreciate: It’s been around for decades, so there’s a long track record. Many users report feeling like their sleep quality improves, not just their sleep quantity. It’s not a controlled substance.
Common experiences: Some users notice mild grogginess in the first hour after waking, especially when starting out. This often improves with timing adjustments—taking it a bit earlier relative to your target wake time.
Why fit still depends on clinician review: Trazodone interacts with certain other medications, and the right dose varies from person to person. Your provider will review your full picture before determining if this option makes sense.
Hydroxyzine
What it is: An antihistamine that’s been used for decades to treat anxiety and allergic reactions. For sleep, it’s often prescribed under the brand name Vistaril.
What kind of sleep problem it’s commonly discussed for: People whose main barrier to sleep is a racing mind—anxiety, mental hyperactivity, or the inability to “turn off” after a high-stress shift. If you lie awake replaying conversations or running through tomorrow’s tasks, this category often comes up.
What people tend to appreciate: It works relatively quickly (often within 30 minutes), and the calming effect can be helpful for both falling asleep and reducing nighttime anxiety. It’s not a controlled substance.
Common experiences: Some users experience morning tiredness or a groggy feeling, as hydroxyzine can stay in your system for an extended period. This sometimes improves with timing adjustments—taking it a bit earlier in your pre-sleep window—though your provider may need to adjust the dose if the fog lingers.
Why fit still depends on clinician review: Your provider will review your medical history and current medications to confirm hydroxyzine is a good match for your situation.
Clonidine
What it is: Originally a blood pressure medication, clonidine calms the sympathetic nervous system—the “fight or flight” response that can keep you wired even when exhausted.
What kind of sleep problem it’s commonly discussed for: The “wired but tired” pattern. If your body is exhausted but your nervous system is still running hot—heart rate elevated, mind alert, unable to physically settle—clonidine addresses that hyperarousal state.
What people tend to appreciate: While it does produce central sedation, it also specifically dials down the physical activation—like a racing pulse or physical restlessness—that prevents natural sleep. Instead of just heavily sedating you, it helps calm the central nervous system’s hyperarousal. Many users report feeling clearer-headed in the morning compared to traditional sedatives. It’s not a controlled substance.
Common experiences: Some users notice mild dry mouth or feel a bit lightheaded when standing up quickly, especially at first. These effects are typically manageable and often diminish over time.
Why fit still depends on clinician review: Your provider will review your health history to confirm clonidine is appropriate for you.
Who’s a Good Fit for Online Treatment
Online sleep treatment is designed for adults between 18 and 65 with schedule-driven or stress-related insomnia who don’t have major medical, psychiatric, or substance-use concerns requiring closer monitoring. You should not be pregnant or planning to become pregnant, and you shouldn’t already be on daily sleep medications or benzodiazepines.
If you fit this profile and have uncomplicated insomnia tied to your work schedule, stress levels, or difficulty winding down, asynchronous or telehealth-based care can be a practical option.
When local evaluation comes first: Some conditions need in-person workup before online medication treatment—including suspected narcolepsy, REM sleep behavior disorder, restless legs syndrome, or sleep apnea (heavy snoring, gasping, breathing pauses). If you’re under 18, over 65, pregnant, or have significant medical or psychiatric concerns, in-person care is the appropriate starting point.
This isn’t about gatekeeping—it’s about matching the right level of care to the right situation.
What Getting Help Actually Looks Like
If you’ve decided to explore non-habit-forming sleep medication through an online platform, here’s how the process typically works:
Digital assessment. You complete an intake questionnaire covering your sleep patterns, medical history, current medications, and any symptoms that might suggest you need a different care path. This isn’t a personality quiz—it’s a clinical screening tool.
Physician review. A licensed provider reviews your information. This is where the actual clinical decision-making happens. The physician determines whether you’re a good candidate for this type of treatment, which medication might fit your pattern, and what dose makes sense to start.
AI tools may help organize information and streamline the workflow, but a real doctor makes the treatment decision. If your case raises questions, you may be asked to complete a brief video visit before any prescription is issued. Some states require a live telehealth visit due to local regulations, while others allow text-based asynchronous care for uncomplicated cases.
Prescription to your pharmacy. If treatment is appropriate, your prescription is often sent electronically to your preferred pharmacy the same day. You pick it up (or have it delivered) just like any other prescription.
Follow-up as needed. Good care doesn’t end at the first prescription. If you need dosing adjustments, have questions about timing, or want to explore a different option, follow-up communication is part of the process.
The whole point of this model is that it works around irregular schedules. You don’t need to take a day off for a 15-minute appointment three weeks from now. You can complete your intake at 2 AM after your shift, and a physician reviews it during business hours. For people whose jobs make traditional clinic hours nearly impossible, this accessibility matters.
For a more detailed walkthrough, here’s what to expect from a safety-first telehealth sleep consult. You can also learn more about how asynchronous care works if you want to understand the difference between text-based and live-visit pathways.
Your Next Step
If you’ve read this far and you’re thinking, “This sounds relevant, but I’m not sure where to start”—you have a few options.
Ready to get started?
You can begin your sleep treatment now. The intake takes about 10 minutes, and a physician reviews your information to determine the best path forward.
Want a quick gut-check first?
The 6-Second Sleep Check helps you see whether your sleep situation warrants further exploration—no commitment required.
Prefer a bit more insight before deciding?
Take the Sleep Clarity Quiz—it takes about 2 minutes and helps you identify what might be driving your sleep issues.
Frequently Asked Questions
Are non-habit-forming sleep meds really non-addictive?
They generally don’t carry the same high abuse risk as controlled substances. Medications like trazodone, hydroxyzine, and clonidine work through mechanisms that don’t typically create the psychological cravings that define addiction, though your body can still build a tolerance, and some require gradual tapering to avoid physical rebound effects. The key distinction is that these options don’t affect your brain’s reward system the way benzodiazepines or Z-drugs can.
Will I feel groggy in the morning?
It depends on the medication, the dose, your timing, and your individual response. Some people experience initial morning grogginess that improves as they dial in the right timing. Others feel clear from the start. Working with a clinician to adjust when you take the medication, or modifying your dose if you are taking a longer-acting option like hydroxyzine, generally helps manage or resolve this.
Is a real doctor reviewing online treatment?
Yes. Licensed physicians review your intake information and make the actual prescribing decisions. AI tools may help organize data or streamline administrative workflow, but a human clinician is responsible for determining whether treatment is appropriate for you. If your situation raises questions, you may be asked to complete a video visit for additional evaluation.
Can shift workers use online care?
Online care works well for people with irregular schedules. You can complete an intake at 3 AM if that’s when you’re awake. Physician review happens during business hours, and prescriptions are sent to your pharmacy electronically. There’s no need to take time off work or sit in a waiting room during hours that don’t match your life.
When should I get checked in person instead?
If you have symptoms suggesting narcolepsy, REM sleep behavior disorder, restless legs, or possible sleep apnea, you’ll want in-person evaluation first. The same applies if you’re pregnant, under 18, over 65, or have significant medical, psychiatric, or substance-use concerns.
Disclaimer: This article is for educational purposes only and is not personal medical advice. Sleep medications are not right for everyone. If you are pregnant, under 18, over 65, have major medical, psychiatric, or substance-use concerns, or have symptoms such as snoring/gasping, daytime sleep attacks, dream enactment, or restless legs, seek local medical evaluation before pursuing online treatment.
Our Editorial Process:
Our expert team uses AI tools to help organize and structure our initial drafts. Every piece is then extensively rewritten, fact-checked, and enriched with first-hand insights and experiences by expert humans on our Insights Team to ensure accuracy and clarity.
By: SleepScriptMD Insights Team
Reviewed by: David Danish, MD, Chief Psychiatric Officer, and Peter Kelly, DO, Chief Medical Officer. Dr. Danish is double board-certified in adult and child/adolescent psychiatry, and Dr. Kelly is a board-certified family medicine physician with over 10 years of clinical practice.