📌 Key Takeaways
A structured 60-minute wind-down routine after your shift matters more than what you do at bedtime.
- Start at Clock-Out, Not Bedtime: Your sleep success depends on the hour after your shift ends—not on trying to relax once you’re already in bed.
- Close the Mental Loop First: Write down what you finished and what’s left for next shift; this tells your brain “work is done” so it stops replaying the day.
- Dim Everything Immediately: Bright lights, phone screens, and overhead fluorescents keep your brain in alert mode—switch to dim lamps the moment you walk in.
- Time Medication After the Downshift: If hydroxyzine is prescribed, take it after you’ve stopped work inputs—it works best when your body is already calming down.
- Protect at Least 6–8 Hours: Morning grogginess usually means the timing was off; don’t take hydroxyzine unless you have a full sleep window before your alarm.
Routine beats willpower—make the first hour boring, dim, and predictable.
Nurses working 12-hour shifts who struggle with post-shift wired-but-exhausted insomnia will find a ready-to-use protocol here, preparing them for the detailed timeline that follows.
~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~
You finished a 12-hour shift. You’re exhausted. But your brain won’t stop running—replaying charts, alarms, the patient in room 4. Generic sleep advice (“just relax”) doesn’t work because it ignores your post-shift adrenaline spike. This guide gives you a structured 60-minute wind-down routine from clock-out to lights-out, plus practical guidance on timing hydroxyzine (when prescribed) so it helps without leaving you foggy for tomorrow’s shift. The goal: a fast, repeatable “hard reset” from hospital mode to sleep mode.
Why the Last Hour After a 12-Hour Shift Decides Your Sleep
You’re sitting in your car in the driveway. Engine off. Too wired to go inside.
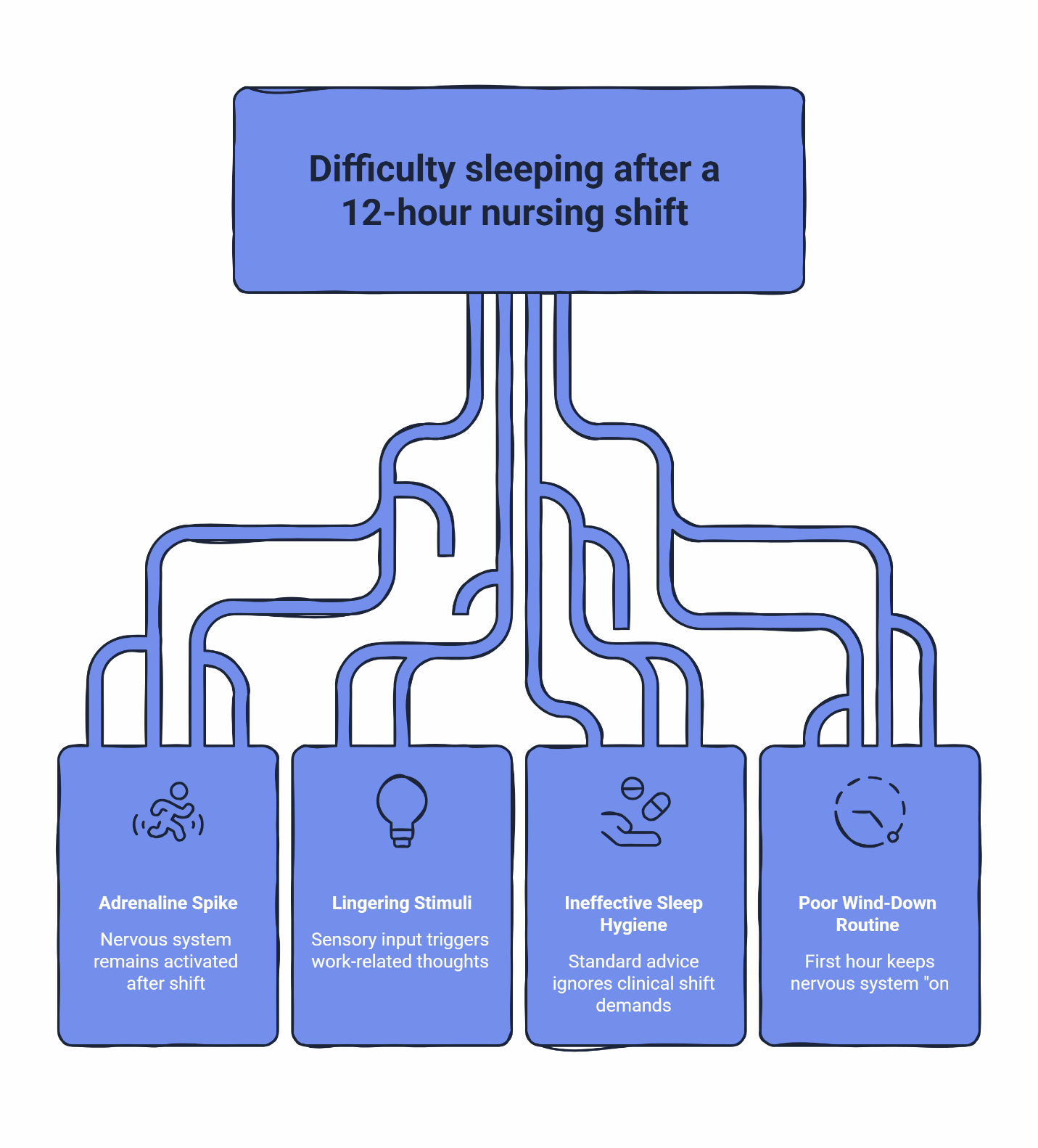
Your body is done. Twelve hours of decisions, alarms, codes, and charting—and now it’s begging for sleep. But your nervous system didn’t get the memo. It’s still running at full speed, replaying every patient interaction, mentally double-checking that last medication you hung. The lingering smell of sanitizer on your scrubs can trigger a full replay of the shift: every chart you updated, every call you made, every “did I miss something?” moment.
This is the “wired but exhausted” state. And it’s why telling yourself to “just relax” feels like an insult.
You’re not “bad at relaxing.” After a 12-hour shift your brain is still running on adrenaline, bright lights, alarms, and nonstop decision-making—so when you finally stop moving, your body feels exhausted but your nervous system stays switched on. The goal of a post-shift routine isn’t a spa night; it’s a fast, repeatable downshift that closes the work loop, blocks new stimulation, and sets a clear boundary between “hospital mode” and “sleep mode.” When hydroxyzine is part of your plan (as prescribed), it tends to work best when you take it inside that calm-down window—after you’ve shut off work inputs—so the medication can meet a body that’s already heading toward sleep, not fighting to stay alert.
The “Golden 60 Minutes” is real. Most nurses don’t lose sleep because they don’t know what blackout curtains are. They lose sleep because the first hour after shift accidentally keeps the nervous system “on”: scrolling under bright kitchen lights, answering unit texts, rehashing the code, eating a heavy meal, or trying to finish charting at home.
Standard sleep hygiene advice fails nurses because it ignores the massive adrenaline spike of a clinical shift. Your sleep success isn’t decided at bedtime. It’s decided in the 60 minutes between clocking out and getting into bed.
“This isn’t sleep hygiene. This is a nervous-system downshift.”
Before You Try Hydroxyzine: Quick Safety Basics
Hydroxyzine (brand name Vistaril) is a prescription medication—a first-generation antihistamine that blocks H1 histamine receptors associated with wakefulness. It’s used off-label for sleep because it produces calming, sedative effects without the addiction risk of controlled substances. Off-label prescribing is a common clinical practice when evidence and safety support it, and a clinician should direct dosing and timing.
Check with your clinician first if you:
- Are pregnant or planning pregnancy (SleepScriptMD does not treat these patients)
- Have heart rhythm concerns, including long QT syndrome
- Are over 64
- Take other sedating medications
Practical guidelines:
- Avoid alcohol while taking hydroxyzine—it increases sedation.
- Don’t drive or work a safety-critical shift until you know how this medication affects you.
- Inform your provider about all medications you currently take.
If you snore, gasp, or stop breathing in sleep: You can still continue an intake with SleepScriptMD, but medication isn’t prescribed until an at-home sleep test is completed and the results are reviewed.
SleepScriptMD does not prescribe benzodiazepines (like Xanax or Ativan) or Z-drugs (like Ambien or Lunesta). Hydroxyzine is a non-addictive sleep medication with no known potential for physical dependence—though it still requires clinician oversight.
The Nurse’s 60-Minute Wind-Down: A Timeline from Clock-Out to Lights-Out
This is your structured protocol. Not suggestions—actions. Each step is designed to down-regulate your nervous system so that by the time you’re ready for bed, your body is already heading toward sleep.
T-60: Clock-Out Boundary (At the Hospital)
Goal: Stop feeding your brain “unfinished business.”
Close the loop. Before you leave the unit, take 90 seconds to write down anything still “open” in your head. Use this specific format:
- 1 sentence: “My shift is over.”
- 3 bullets: What you completed.
- 1 bullet: One thing for next shift.
This signals to your nervous system: shift is done. Get it out of your brain and onto paper (or a note on your phone).
Put your phone on Do Not Disturb. Set an auto-reply for work texts: “Off shift. Will respond tomorrow.” Silence unit group texts, turn off email notifications, and pick one decompression cue you will repeat every time—the same playlist, the same podcast, or silence.
T-45: The Commute (Nervous-System Downshift)
Goal: Shift from alert scanning to steady.
Your commute is not for doomscrolling or catching up on messages. It’s part of the routine.
- Audio: Switch to something low-stimulation—a calm podcast, instrumental music, or silence. No news. No work calls. No scrolling at red lights.
- Lighting: If it’s daylight, wear sunglasses. Bright light keeps your brain alert. If it’s night, dim dashboard lights.
- Temperature: Cool the car down slightly. A drop in body temperature signals sleep is coming.
- Breathing: Inhale through the nose, slow exhale, repeat. A pattern you can actually do while driving.
The commute is your transition zone. Treat it like one.
T-30: Home Entry (Dark, Quiet, Cool)
Goal: Your home should feel like a different planet than the unit.
Walk in the door and immediately signal “sleep mode” to your environment:
- Dim the lights. No overhead fluorescents. Warm, dim lamps only—or keep lights off entirely.
- Shower or wash your face. Get the hospital off your skin. Even 2 minutes removes the “hospital smell” and gives your brain a sensory reset. The water temperature shift also helps your body start cooling down.
- Put your phone in another room or on a charger away from your bed.
If you’re hungry, keep it light—a small snack with protein or complex carbs. Nothing heavy, nothing sugary.
T-20: Set the Sleep Environment
Goal: Remove the friction points that steal 30 minutes later.
- Blackout curtains closed.
- Fan or white noise on.
- Phone face-down (or better, in another room).
- Room cool (65–68°F is ideal).
- Bed is for sleep only—no charting, no case review, no “one more thing.”
T-15: Medication Timing Window (If Prescribed)
Goal: Align the medicine with a nervous system that’s already coming down.
If hydroxyzine is part of your clinician-directed plan, this is your window.
Typical dosing (clinician-directed): 25–100 mg at bedtime. Sedative effects usually begin within 15–30 minutes, according to MedlinePlus. Taking it 30–60 minutes before you want to be asleep gives the medication time to work.
Take it after you’ve shut down work inputs—not while you’re still charting or scrolling. Hydroxyzine works best when it meets a body that’s already winding down, not one that’s still in “hospital mode.”
T-0: Lights Out (Protect the Boundary)
Goal: Don’t renegotiate with yourself.
- Phone on Do Not Disturb.
- One page of something boring or a short audio track if your brain is still revving.
- If you’re awake, keep the room dark and stimulation low.
You’ve closed the loop. Your body is ready.
The Nurse’s 60-Minute Wind-Down Checklist
Screenshot or print this. Follow it after every shift.
Time | Action |
|---|---|
T-60 | Write the “close the loop” note (1 sentence + 3 bullets + 1 bullet). Phone on Do Not Disturb. Silence work notifications. |
T-45 | Commute: low-stimulation audio, sunglasses if daylight, cool car. No scrolling. |
T-30 | Home entry: dim lights immediately, shower or face wash, phone in another room, light snack if needed. |
T-20 | Blackout curtains closed, white noise on, phone face-down, room cool. |
T-15 | Take hydroxyzine (if prescribed). Stay off screens. |
T-0 | Lights out. Do Not Disturb. Bed is for sleep. |
How to Time Hydroxyzine So It Helps—Without Morning Grogginess
The most common complaint? “I took it and felt groggy the next morning.”
Usually, that’s a timing or dose issue—not a sign the medication doesn’t work for you.
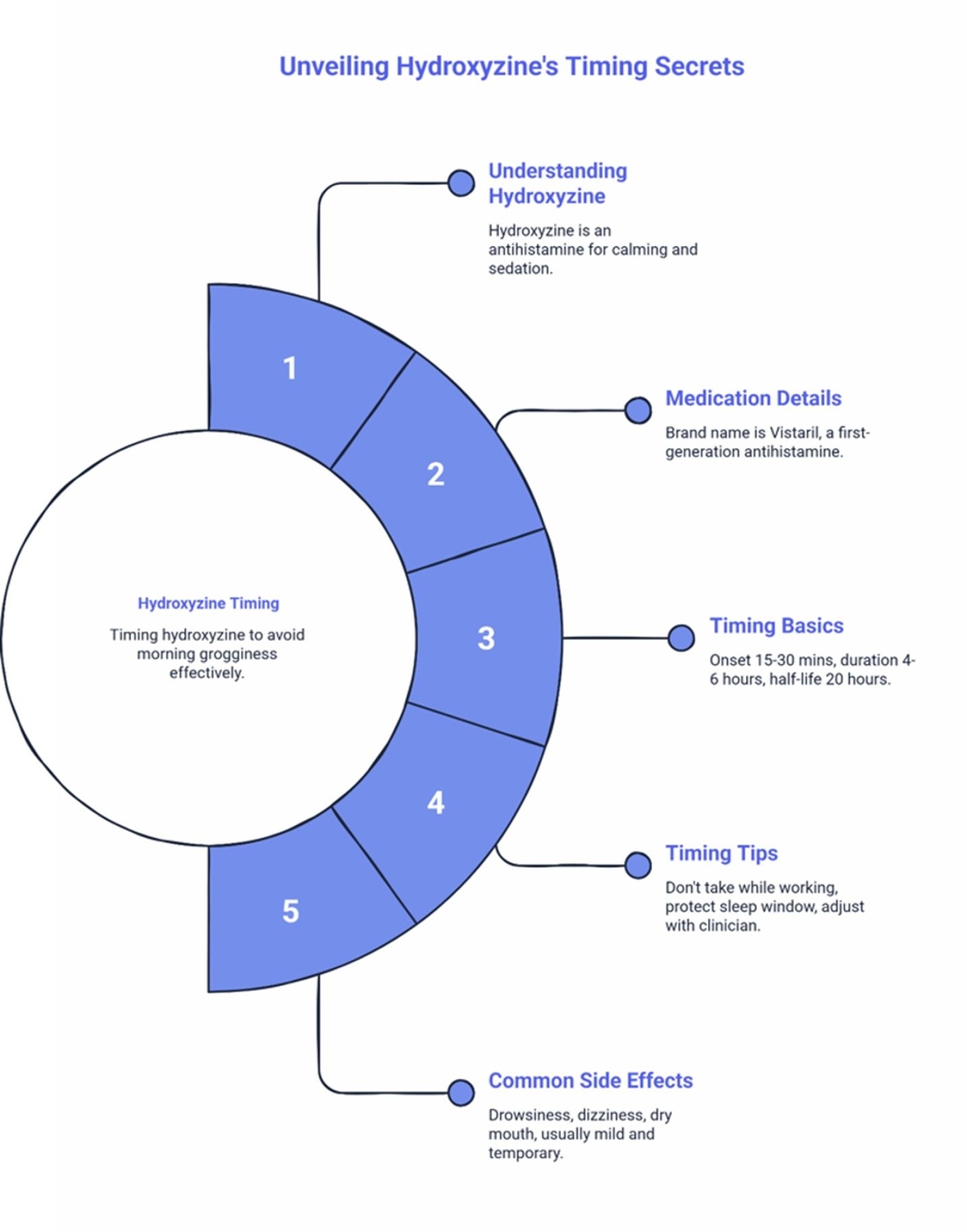
What hydroxyzine is (plain English): Hydroxyzine is a first-generation antihistamine used for its calming and sedating effect. It blocks H1 histamine receptors associated with wakefulness, helping reduce mental arousal without engaging the GABA pathways that cause addiction with benzodiazepines and Z-drugs.
Medication details: Brand name is Vistaril.
Timing basics that matter for nurses:
- Onset: Hydroxyzine typically produces sedative effects within 15–30 minutes.
- Duration: Peak sedative effects generally last 4–6 hours, though the medication has a long metabolic half-life (up to 20 hours), which necessitates careful timing to avoid morning grogginess.
- Common timing: Many people take it 30–60 minutes before bedtime (clinician-directed).
Timing Tips for Clear Mornings
1) Don’t take it while you’re still in work mode.
If you’re charting, texting coworkers, or replaying the shift, you’re still feeding arousal. Do the boundary steps first, then take it.
2) Protect a real sleep window.
If you have to drive or function in a safety-critical role soon after waking, you need to learn how the medication affects you before you rely on it on a tight turnaround. Don’t take hydroxyzine unless you have at least 6–8 hours before your alarm.
3) If you feel groggy, adjust with your clinician.
If you’re waking up foggy, try taking it 15–30 minutes earlier in the evening. This gives your body more time to metabolize the medication before your alarm goes off. Timing shifts and dose adjustments are common clinician tools to reduce morning tiredness.
One patient put it this way: “I’ve tried a bunch of different things for my sleep, and most of them either didn’t work or made me feel like a zombie the next day.” The difference with hydroxyzine, when timed correctly, is that it can help you fall asleep faster without the heavy sedation of controlled options.
Common side effects include drowsiness, dizziness, and dry mouth. These are typically mild and often improve as your body adjusts.
For a public-facing medication reference, see MedlinePlus drug information for hydroxyzine.
Troubleshooting: When You’re Still Wired (Or When It’s Not Adrenaline)
Sometimes the routine helps but something else is getting in the way. Use this section like a decision tree.
Common Friction Points (Fixable Tonight)
If you’re still wired, check these first:
- Charting at home. If you’re finishing notes after shift, you’re staying in work mode. Your nervous system doesn’t know the shift is over.
- Doomscrolling. Social media and news feeds are designed to keep you alert. They work.
- Late-shift caffeine. That last coffee at hour 10 is still in your system. Caffeine typically has an estimated half-life of about 5 hours, though this can vary widely depending on your individual metabolism.
- Bright light exposure. Overhead lights, phone screens, and even the bathroom light can suppress melatonin and keep your brain in “daytime” mode.
- Notification drip. “Just checking” messages keeps your brain scanning for problems.
Fast fixes:
- Move the phone charger outside the bedroom.
- Replace overhead lighting with one dim lamp.
- Make the shower the “line in the sand” between work and sleep.
When to Seek In-Person Evaluation
Not all sleep problems are adrenaline. If you’re experiencing any of the following, you may have a condition that requires in-person evaluation:
Snoring, gasping, or stopping breathing during sleep. You can still start the SleepScriptMD intake process, but an at-home sleep test is required before any medication is prescribed.
Sudden daytime sleep attacks or muscle weakness with strong emotions. These may be signs of narcolepsy, which requires in-person evaluation and a full sleep study. The Narcolepsy Network Resource Center has resources for next steps.
Acting out dreams physically (yelling, kicking, punching while asleep). This may indicate REM sleep behavior disorder, which requires specialty evaluation.
Uncontrollable urge to move your legs at night. Restless legs syndrome often needs lab work and in-person evaluation.
These conditions can’t be safely treated through telehealth alone. If any of these apply, please seek in-person evaluation with a local sleep specialist.
Make It Automatic: The 3 Triggers That Turn This Into a Habit
You protect patients by following protocols. Protect your recovery the same way.
Trigger 1: Environmental Sequence
Do the same thing in the same order every time. Clock out → write down open loops → phone on DND → commute with calm audio → dim lights at home → shower → medication (if prescribed) → bed. Your brain learns: this sequence means sleep.
Trigger 2: Phone Boundary
Your phone is the biggest threat to your downshift. Auto-reply is set. Do Not Disturb is on. The phone is charging in another room. This is non-negotiable. If you keep your phone nearby, you keep “work brain” nearby.
Trigger 3: Bed Is Only for Sleep
No charting in bed. No scrolling in bed. No “just checking one thing” in bed. When your body hits the mattress, it knows exactly what’s supposed to happen next. If you’re awake, keep the room dark and stimulation low.
Consistency is what makes this work. One patient described it this way: “I have a crazy work schedule and no time for doctor appointments. This was the easiest thing ever—filled out some questions, got approved, and my prescription was ready pretty fast. I don’t wake up a million times a night anymore.”
If You Want Clinician-Guided, Non-Addictive Options
If you’re ready to talk to a clinician about whether hydroxyzine or another non-controlled option fits your situation, SleepScriptMD offers a streamlined path.
How It Works
- Check eligibility and complete a 10-minute assessment. You’ll answer questions about your sleep patterns, medical history, and current medications. Information can be organized by AI to flag safety concerns.
- Physician review. A licensed provider reviews your information and medical history. Every prescription is individually reviewed and approved by a physician—this isn’t algorithm-only care. The physician makes an independent clinical decision about whether treatment is appropriate.
- Prescription sent to your pharmacy (if appropriate). If you’re eligible, your prescription is often sent electronically to your preferred pharmacy the same day in most states. Medication cost is separate and paid at the pharmacy—SleepScriptMD does not sell medications.
- Follow-up and refills. Ongoing care is available via text-based check-ins or telehealth visits for more complex cases.
Which Care Path Fits?
- Text-based care: Complete the assessment on your own time; clinician review happens asynchronously. Available in most states.
- Telehealth visit: A live video session for people who prefer direct interaction or have more complex histories. Required in some states.
Compare text-based care vs. telehealth visits
SleepScriptMD is a self-pay service and does not bill insurance directly. For current details, visit the pricing page.
If you have unique circumstances or don’t meet standard eligibility criteria, you can reach out directly at Admin@SleepScriptMD.com.
Next Steps (Pick the One That Matches Your Situation)
Ready to get started? Check eligibility and start your 10-minute assessment
Want to learn more about hydroxyzine specifically? Hydroxyzine for sleep prescription online
Want to compare medication options? Medication Selection Page
Looking for the broader approach to non-addictive options? Safe, Non-Addictive Prescription Sleep Aids
Not sure which direction to go? Choose your sleep quiz
Trust and Transparency
- LegitScript verification
- Healthgrades – Dr. Peter Kelly, DO
- Healthgrades – Dr. David Danish, MD
- Doximity – Dr. Peter Kelly, DO
Bottom Line
You protect patients all shift long. This is how you protect recovery. Start your routine at clock-out, not at bedtime. Make the first hour boring, dim, and predictable—then (if hydroxyzine is part of your prescribed plan) let timing do its job.
Start your 10-minute assessment
Disclaimer: This article is for educational purposes only and does not replace medical advice. Hydroxyzine is a prescription medication and is not appropriate for everyone. Do not start, stop, or change any medication without guidance from a licensed clinician. If you have symptoms that suggest another sleep disorder, seek in-person evaluation with a local clinician or sleep specialist.
Our Editorial Process:
Our expert team uses AI tools to help organize and structure our initial drafts. Every piece is then extensively rewritten, fact-checked, and enriched with first-hand insights and experiences by expert humans on our Insights Team to ensure accuracy and clarity.
About the SleepScriptMD Insights Team:
The SleepScriptMD Insights Team is our dedicated engine for synthesizing complex topics into clear, helpful guides. While our content is thoroughly reviewed for clarity and accuracy, it is for informational purposes and should not replace professional advice.