 Key Takeaways
Key Takeaways
 Key Takeaways
Key TakeawaysPlan your sleep medication around when you need to be alert, not when you happen to get home from work.
- Work Backward From Wake Time: Count hours backward from when you must be clear-headed—your drive to work or first task—then place your medication 30-60 minutes before intended sleep.
- Swing Days Need Extra Care: When your schedule flips dramatically, extend your safety buffer or skip the dose entirely if you have less than 6-7 hours before driving.
- Track Your Clarity Score: Rate your morning alertness 1-10 for 5-7 days to spot patterns—most timing problems fix themselves with a 15-30 minute shift earlier or later.
- Different Medications Clear Differently: Hydroxyzine and clonidine often work within 30-60 minutes; trazodone helps you stay asleep but may need more clearance time before your alarm.
- Protect Real Sleep Blocks: Your actual sleep window shrinks after commute, shower, and wind-down—calculate what you truly have, not what the clock says.
Clear mornings come from planning tonight’s dose around tomorrow’s demands.
Shift workers juggling rotating schedules will gain a repeatable timing system here, preparing them for the detailed medication-specific guidance that follows.
~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~
You look at tomorrow’s schedule. Then the clock. Then the pill bottle. Your shift flips from nights to days in 36 hours, and you have a narrow window to get this right.
The standard advice — “take it at bedtime” — falls apart when bedtime itself keeps moving. A rotating schedule means your medication timing has to slide with it. Otherwise you wake up foggy during a shift that demands you be sharp, or you lie awake during the only sleep window you have.
If over-the-counter products have already left you with a zombie hangover, that frustration makes sense. Rotating shifts fight the light-dark cycle that drives circadian rhythms, and changing work times makes changing sleep times harder in the first place.
This isn’t about finding the perfect dose. It’s about learning to think backward from when you need to be alert, protecting your sleep blocks, and knowing exactly when to check with your provider for guidance on a specific transition.
Why a 3-Day Rotating Shift Breaks the Usual “Take It at Bedtime” Rule
Rotating schedules work against your body’s internal clock in ways that fixed shifts don’t. Your circadian rhythm — the 24-hour cycle that tells you when to sleep and when to wake — is anchored to light and darkness. When your work schedule keeps flipping between day and night shifts, that anchor gets pulled around constantly.
The AASM provider fact sheet on shift work explicitly confirms this pattern: workers on rotating shifts experience longer sleep latency, more awakenings, more excessive sleepiness, and more work-related accidents than workers on fixed day or night schedules. The American Academy of Sleep Medicine (AASM) clinical practice guidelines confirm that symptoms of shift work disorder often stem from misalignment between the body’s internal clock and the required work schedule.
The result is predictable. You’re exhausted but wired. You finally get home and your body doesn’t believe it’s time to sleep. Then the medication you took at “bedtime” is still lingering when your alarm goes off, because bedtime last night was 7 AM and bedtime tomorrow will be 11 PM.
Fixed-shift workers can memorize a single timing routine. You can’t. Your medication timing needs to move every time your schedule moves.
Start With Your Next Required Wake Time, Not the Clock on the Wall
The most common timing mistake is thinking about when you’re going to bed instead of when you need to be awake and functional.
Here’s the shift in thinking: work backward from the moment you absolutely must be clear-headed. That might be the start of your next shift. It might be the drive to work. It might be a safety-critical task in the first hour. Whatever it is, that’s your anchor point.
The wake-time-backward method:
- Identify your next required wake time — the latest moment you can be asleep and still function safely
- Count backward to find how many hours of sleep opportunity you actually have
- Place your medication window far enough before intended sleep that the medication has time to work, but not so early that it wears off mid-sleep
For most non-addictive sleep medications, this means taking the dose 30-60 minutes before you intend to fall asleep. But the critical variable is what happens on the other end. If you need to be alert at 6 AM and your medication tends to leave you groggy for 7-8 hours after taking it, you shouldn’t be taking it at 1 AM.
Your sleep block is not the same as “time at home.” It’s the real block left after the commute, food, shower, blackout curtains, and the 20 minutes where you stare at the ceiling because your brain is still in work mode.
A nurse finishing a 7 PM to 7 AM shift might get home at 7:45 AM and need to sleep until 4 PM for the next night shift. That’s roughly 8 hours of sleep opportunity. She can take her medication around 8 AM and expect to wake up clear. But if she works an evening shift that ends at 11 PM and her next shift starts at 7 AM the following morning—meaning she must be awake by 5:30 AM—taking medication at 1 AM leaves only 4.5 hours for clearance. That math guarantees a chemical hangover.
The same approach applies to an industrial worker flipping from an evening shift to an early start, or a 7-on/7-off worker trying to reset after a run of nights. Different jobs, same logic: protect your next wake time first.
The 3-Day Rotating Shift Timing Framework
This framework assumes you’re already working with a provider who has prescribed a non-controlled sleep medication like trazodone, hydroxyzine, or clonidine. The goal here is timing logic, not medication selection.
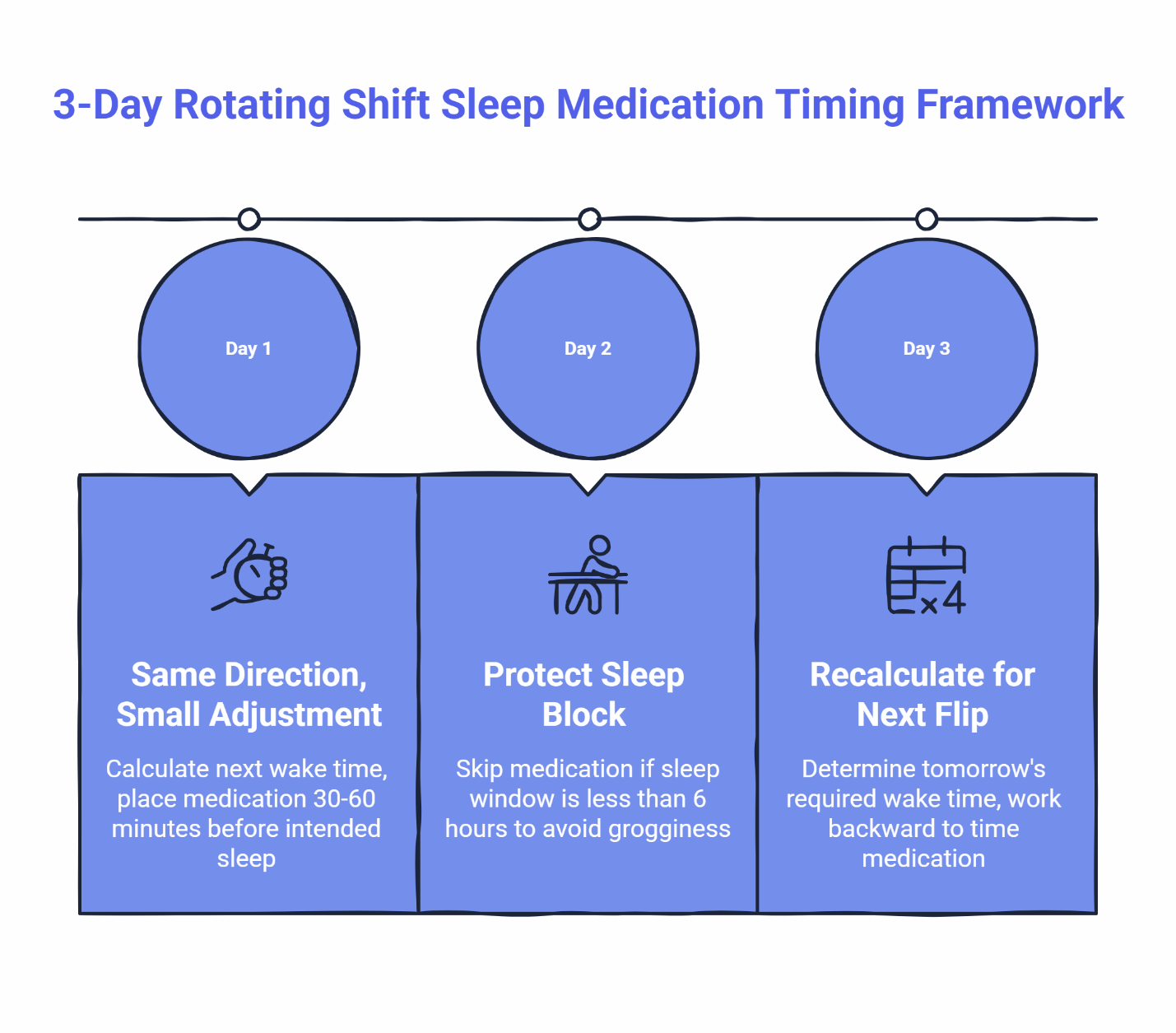
Day 1: Same general direction, small adjustment
On the first day of your rotation block, your body still remembers the previous schedule. If you’re shifting from nights to days, your internal clock is still expecting to sleep during daylight hours.
Calculate your next required wake time. Count backward to find your sleep opportunity. Place your medication in the same relative position you used before — usually 30-60 minutes before intended sleep. The main adjustment is the clock time, not the spacing.
Day 2: Protect the sleep block
By day two, you’re deeper into the new schedule but your body hasn’t fully adjusted. This is when people start making timing errors out of frustration.
The rule here: protect the sleep block you have. If a brutal turnaround leaves you with only 6 hours between shifts, taking a standard prescription sleep aid is a critical safety hazard. In these heavily compressed windows, you must skip the medication entirely to avoid life-threatening grogginess during your commute.
A common pitfall is treating the medication like an on-demand add-on after a long scroll, late meal, or second wind. That’s how you drift too close to tomorrow’s alarm.
Day 3: Recalculate because the schedule moved again
If you’re on a true 3-day rotation, day three often means preparing for another schedule flip. This is where wake-time-backward thinking matters most.
Before you take anything, ask: “When do I absolutely need to be alert tomorrow?” Then work backward from there. If the math doesn’t leave enough clearance, that’s a signal to either skip the dose or contact your provider for guidance.
The consistency principle
Across all three days, try to keep the relative timing consistent even when the clock times change. If your pattern is “medication 45 minutes before intended sleep, with at least 7 hours before I need to drive,” maintain that ratio. Your body starts to recognize the pattern, and sleep onset often gets faster over 5-7 days of consistent use.
Five-step flow for every rotation
- Identify your next required wake time
- Identify your real sleep opportunity
- Decide whether this is a normal rotation day or a swing day
- Place the medication timing window before intended sleep, not by habit
- Log sleep onset and wake clarity the next day
That’s the whole system. Clean. Repeatable. Useful.
How to Handle the Swing Day
The swing day — the transition between schedule blocks — is where timing matters most.
On a swing day, your sleep window is often compressed, your wake time is shifting dramatically, and the temptation to “just take something” is highest. This is also when getting the timing right makes the biggest difference.
Swing day guidelines:
First, calculate your actual sleep opportunity. If you’re transitioning from nights to days, you might have an unusually short or long sleep block depending on how the schedule falls. Know the exact number of hours before you reach for the medication.
Second, consider a slightly earlier cutoff. On normal rotation days, you might be comfortable with 7 hours between medication and wake time. On a swing day, extending that to 8 hours can help account for the additional fatigue from the schedule change itself.
Third, if the math doesn’t work, check with your provider. If your swing day only gives you 4 hours of sleep opportunity before you need to drive or work, your provider can help you decide whether to skip the dose, adjust the timing, or use a different approach for that specific transition.
One more factor worth knowing: the AASM notes that counter-clockwise rotations — flipping backward from night to evening to day — tend to be harder than clockwise ones. If your schedule rotates in that direction, a bit more planning helps.
Quick check: If your sleep window before driving or work is shorter than the typical duration of your medication’s effects, reach out to your provider for guidance on that specific transition day.
How Trazodone, Hydroxyzine, and Clonidine Timing Can Differ
Which medication is right for you depends on your health history, other medications, and your provider’s assessment. What matters here is understanding that different medications have different timing characteristics.
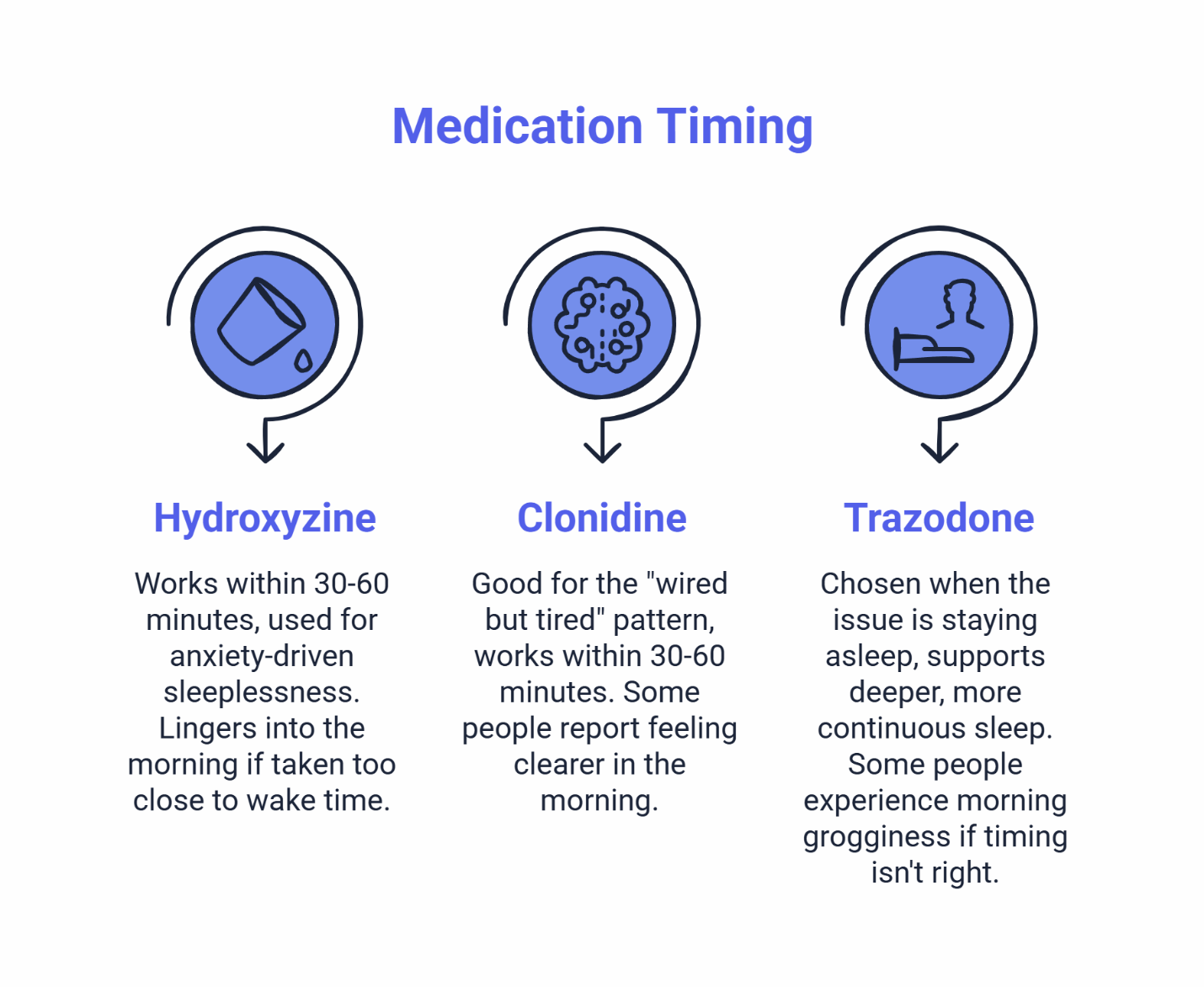
Hydroxyzine often works within 30-60 minutes and is commonly used for anxiety-driven sleeplessness or racing thoughts. Some users find it lingers into the morning if taken too close to wake time. Shifting the dose 15-30 minutes earlier often helps — but any adjustment should be discussed with your provider. If you’re a nurse working long shifts and hydroxyzine is part of your plan, the post-12-hour-shift wind-down routine for nurses using hydroxyzine can help you think through the transition from clock-out to sleep.
Clonidine is often a good fit for the “wired but tired” pattern — when you’re exhausted but your mind won’t stop racing, especially with stress-related insomnia or ADHD-related sleep disruption. It tends to work within 30-60 minutes as well. Some people report feeling clearer in the morning compared to other options. Common side effects like dry mouth or mild dizziness typically fade as your body adjusts.
Trazodone is often chosen when the issue is staying asleep, not just falling asleep. It supports deeper, more continuous sleep for many users. The tradeoff is that some people experience morning grogginess if the timing isn’t right. Getting the timing window dialed in matters more with trazodone because of that potential for lingering sedation.
The common thread: all three work well when you protect enough time between the dose and your next alert period. The specific number of hours varies by person and by medication, which is why tracking matters.
What to Track for 5-7 Days So You Can Fine-Tune
Most timing issues are solved by small adjustments — often 15-30 minutes earlier or later — not by abandoning the medication after one rough morning. But you can only make smart adjustments if you know what’s actually happening.
Track these fields for at least 5-7 days:
- Medication time: When you actually took it
- Intended sleep time: When you planned to fall asleep
- Actual sleep onset: When you estimate you actually fell asleep
- Wake time: When you got up
- Wake clarity score (1-10): How clear-headed you felt in the first 30 minutes
- Grogginess duration: How long until you felt fully alert
- Notes: Anything else worth remembering
The pattern usually becomes obvious within a week. If your clarity score drops when you take the medication after midnight but stays high when you take it before 11 PM, that tells you something. If grogginess lasts 90 minutes on nights when you only slept 5 hours but clears in 20 minutes after 7-hour sleep blocks, that tells you something too.
Many timing issues improve with small provider-guided shifts rather than stopping after one rough morning. That fits the broader guidance behind timing windows to avoid next-day grogginess and managing common, mild side effects.
Bring this log to your next check-in with your provider. Small timing shifts — guided by actual data — work better than guesswork.
If you want a quick pattern check before a full intake, the sleep quiz chooser offers a low-friction way to get clear next steps.
Practical Timing Guidelines
Sleep medication is a tool that works best with a little planning. Here’s how to get the most from it.
Timing tips:
- Plan backward from your next required wake time
- Keep your medication list current so your provider can check for interactions
- Track wake clarity for 5-7 days to spot patterns
- Reach out to your provider if you’d like help fine-tuning
What to avoid:
- Taking it just because you’re finally home (timing matters more than habit)
- Combining with alcohol — it can amplify drowsiness
- Using the same timing on a swing day that you use on a stable day without checking the math
Good times to check in with your provider:
- Grogginess that doesn’t improve after the first week of adjustment
- A work schedule so erratic that you can’t establish any consistent timing pattern
- Any questions about how the medication is working for you
This service treats adults 18-65 who are low-risk for complications. We don’t treat certain conditions online, including suspected narcolepsy, REM sleep behavior disorder, or restless legs syndrome — those need in-person evaluation with a local specialist. We also don’t prescribe controlled substances like Ambien or Xanax. If you’ve been told you snore, gasp, or stop breathing during sleep, an at-home sleep test may be needed before medication is prescribed.
A Quick Word on Process
If your case is straightforward, text-based care may be the easiest fit for a demanding work schedule. If it’s more complex, the next step may be a provider text follow-up or a brief virtual session. Some states require a video visit before prescribing — your intake will let you know what applies to you. That’s the basic setup behind how asynchronous care works.
“I have a crazy work schedule and no time for doctor appointments. This was the easiest thing ever—filled out some questions, got approved, and my prescription was ready pretty fast.” — Emily R.
Your Printable 3-Day Rotating Shift Medication Planner
Use this planner to map your medication timing across a full rotation cycle. The goal is to make wake-time-backward thinking automatic.
3-Day Rotating Shift Medication Planner
Day 1
- Next Shift Starts:
- Shift Ends:
- Need to Be Clear-Headed By:
- Intended Sleep Block:
- Medication Timing Window:
- Swing Day: Yes / No
- Wake Clarity Score (1-10):
- Notes:
Day 2
- Next Shift Starts:
- Shift Ends:
- Need to Be Clear-Headed By:
- Intended Sleep Block:
- Medication Timing Window:
- Swing Day: Yes / No
- Wake Clarity Score (1-10):
- Notes:
Day 3
- Next Shift Starts:
- Shift Ends:
- Need to Be Clear-Headed By:
- Intended Sleep Block:
- Medication Timing Window:
- Swing Day: Yes / No
- Wake Clarity Score (1-10):
- Notes:
Fill it out before each rotation block. Start with your required wake times, then work backward to find your medication window. On swing days, be honest about whether the math works — if it doesn’t, your provider can help you figure out the best approach.
Bring your completed planners to your next appointment. The pattern of clarity scores across multiple cycles gives your provider real data to work with.
A 3-day rotating shift can make sleep feel random, but your timing doesn’t have to be random. Protect the next wake time. Plan ahead for swing days. Track what happens for a week. Then adjust with your provider, not by guesswork.
That’s how you get better nights and clearer mornings.
Take the Sleep Clarity Quiz — it takes about 2 minutes and gives you clear next steps plus a printable PDF you can bring to your provider.
Or if you already know you need clinical guidance, start your confidential sleep assessment and connect with a board-certified physician who understands shift work.
Disclaimer: This content is for informational purposes only and does not replace medical advice, diagnosis, or treatment. Sleep medication timing, dose, and appropriateness depend on your health history, other medications, job requirements, and available sleep window. Use sleep medications only under the guidance of a licensed clinician. If you feel sedated, avoid driving or operating machinery until you feel fully alert. Reach out to your provider with any questions about how your medication is working for you.
Our Editorial Process:
Our expert team uses AI tools to help organize and structure our initial drafts. Every piece is then extensively rewritten, fact-checked, and enriched with first-hand insights and experiences by expert humans on our Insights Team to ensure accuracy and clarity.
About the SleepScriptMD Insights Team:
The SleepScriptMD Insights Team is our dedicated engine for synthesizing complex topics into clear, helpful guides. While our content is thoroughly reviewed for clarity and accuracy, it is for informational purposes and should not replace professional advice.