📌 Key Takeaways
Your sleep medication works best when you give it a calm, predictable hour before bed—not a chaotic scroll session.
- Build a Simple Pre-Sleep Runway: Dimming lights, cutting screens, and doing the same few things each night trains your brain that sleep is coming.
- Stack New Habits on Old Ones: Attach tiny sleep-supporting actions to things you already do—like switching your phone to night mode when you set your alarm.
- Cut Caffeine Six Hours Before Bed: Half that afternoon coffee is still in your system when you’re trying to wind down, fighting your medication.
- Skip the Nightcap: Alcohol fragments sleep later in the night and can interact unpredictably with sedating medications.
- Track Your Morning Clarity: Rating how clear you feel each morning (1–10) helps you spot patterns and bring useful info to your clinician.
Small habit shifts amplify what your medication can do.
Shift workers, night nurses, and anyone with an unpredictable schedule will find practical routines here, preparing them for the tracking tools that follow.
~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~
You got home at 7 AM. The blackout curtains are drawn. The melatonin is on the nightstand—again. And your brain? Still running through every conversation from the last twelve hours.
You’ve tried the gummies. You’ve tried the Benadryl. Both left you feeling like a zombie when your alarm went off six hours later, stumbling through the start of your next shift with that foggy, cotton-headed feeling that makes even pouring coffee feel dangerous.
Here’s the thing: if you’ve been prescribed a non-addictive sleep medication like trazodone, hydroxyzine, or clonidine, the pill itself is only part of the equation. What you do in the hour before you take it can make the difference between restless tossing and actual, restorative sleep—and between waking up groggy or waking up clear.
This isn’t about perfect sleep hygiene. It’s about building a simple system that gives your medication a fair shot at working.
The 60-Minute Setup: Why Your Evening Before the Pill Matters
Your medication works best when you give it a clean runway before takeoff. Think of your prescription like a landing plane. The medication isn’t the whole flight plan—it’s the final approach. If the hour before bed is chaotic (bright lights, doomscrolling, heavy food, stress spikes), your brain gets mixed signals: “stay alert” and “go to sleep” at the same time.
Without that runway, even a well-chosen medication has to fight harder to do its job.
Here’s what the runway actually is, in plain terms:
- A predictable “downshift” window before sleep
- A few repeatable cues that tell your nervous system: we’re done for today
- A way to reduce next-day grogginess triggers (late caffeine, alcohol, heavy meals, bright screens)
You don’t need a spa-like ritual. You need a predictable sequence—something your brain learns to recognize as the signal that sleep is coming. According to healthy sleep guidance from the NHLBI, consistency in your pre-sleep routine helps reinforce your body’s natural sleep-wake signals.
Habit Stacking: The Easiest Way to Make a Routine Stick
Habit stacking attaches a tiny new habit to something you already do, so it runs on autopilot.
Instead of building a whole new routine from scratch, you piggyback. You already brush your teeth. You already plug in your phone. You already change out of your scrubs or work clothes. You already lock the door or turn off the kitchen light. These are your anchors.
The trick is picking just two or three anchors and adding one tiny sleep-supporting action to each. That’s it. No elaborate checklists. No guilt when you skip a step.
Focus on execution over optimization. Pick 2–3 anchor habits you already do, then add 1–2 tiny sleep-supporting moves.
If you’ve tried “sleep hygiene” and it felt like a personality transplant, this is the fix: you’re not adding a new lifestyle—you’re piggybacking on your current one.
The 5 Habits That Most Reliably Improve Medication-Supported Sleep
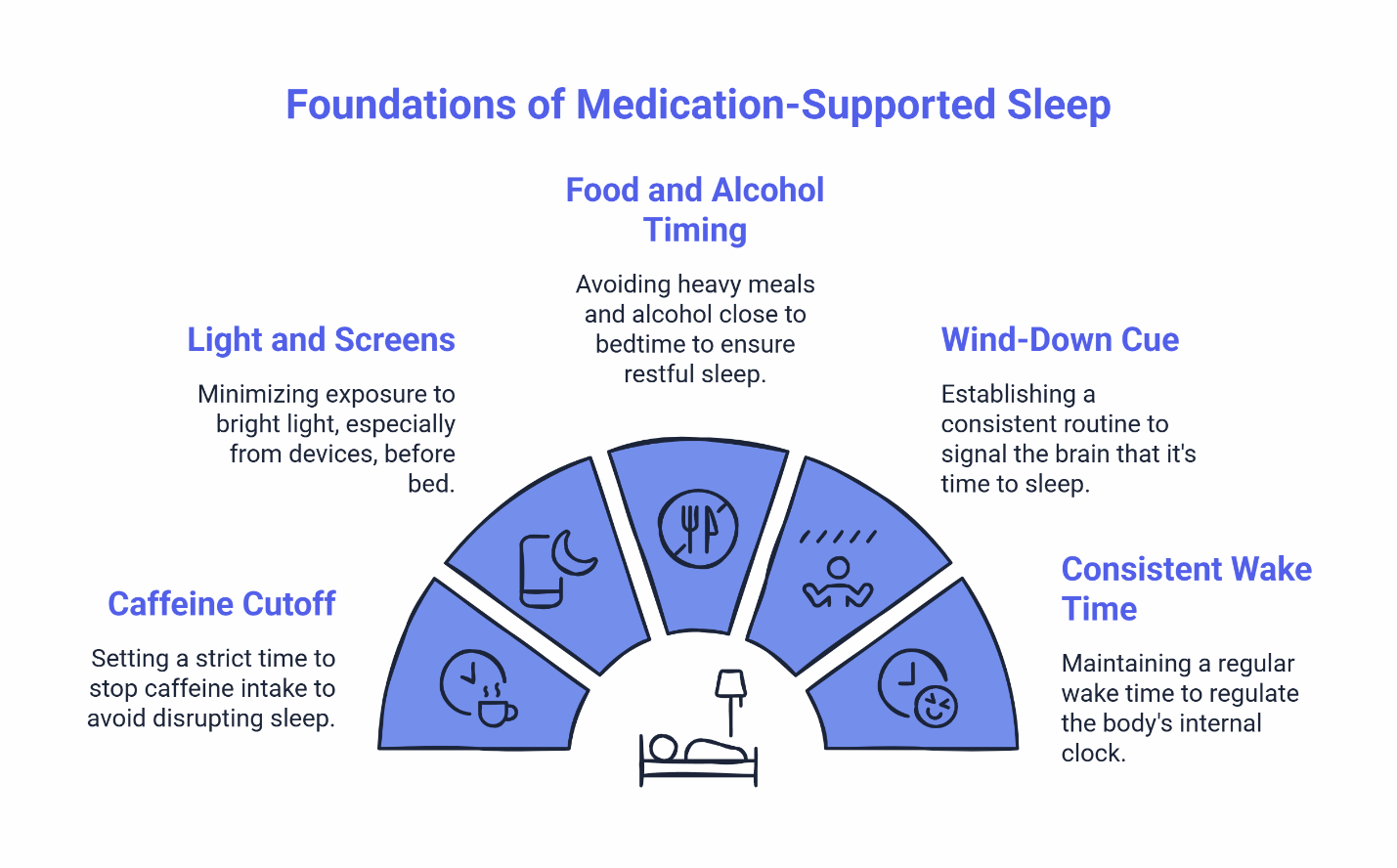
1. Caffeine Cutoff
Why it helps: Caffeine has a half-life of about five hours, meaning half of that afternoon coffee is still circulating when you’re trying to wind down. It can quietly “prop up” alertness longer than you think—especially if you’re using it to survive a shift.
Tiny version: Set a “last call” alarm on your phone—six hours before your target sleep time. When it goes off, switch to water or decaf. Pick a caffeine stop-time that’s realistic for your life (not aspirational), and make it a rule you don’t renegotiate at 2 p.m. when you’re fading.
2. Light and Screens
Why it helps: Bright light—especially the blue-white glow from phones and tablets—tells your brain it’s still daytime. That signal fights directly against your medication’s sedative effect.
Tiny version: Dim the lights in your space and switch your phone to night mode 45 minutes before bed. If you need to scroll, keep the screen brightness at its lowest setting. Or switch to audio (podcast, audiobook) instead of scrolling.
3. Food and Alcohol Timing
Why it helps: A heavy meal keeps your digestive system active when it should be powering down. Alcohol, while sedating at first, fragments sleep later in the night and can interact unpredictably with sleep medications.
Tiny version: Finish eating at least two hours before bed. If you’re hungry late, keep it small and boring (think “snack,” not “meal”). If you drink, keep it early in your off-shift hours—not as a “nightcap.” Skip alcohol close to bedtime, especially with any sedating medication.
4. Wind-Down Cue
Why it helps: Doing the same two or three things every night trains your brain to anticipate sleep. It’s the behavioral equivalent of a biological wind-down. Your brain likes patterns. A repeatable sequence becomes a “now we sleep” trigger—even when your bedtime moves.
Tiny version: Pick a sequence you can repeat anywhere—wash your face, set your alarm, take your medication. Same order, every time. One calm activity helps: stretch for 60 seconds, read 2 pages, or breathe slowly for 1 minute.
5. Consistent Wake Time (or Anchor Wake Time)
Why it helps: Your body’s internal clock anchors more strongly to when you wake up than when you fall asleep. A stable wake time—even on days off—keeps your circadian rhythm from drifting.
Tiny version: Pick a wake time you can hit most days.
The CDC’s sleep guidance reinforces that these basics—light management, caffeine timing, and consistent schedules—form the foundation of sustainable sleep health.
A Shift-Worker Version: When Bedtime Moves but You Still Need a System
If you’re working 7-on/7-off, rotating days and nights, or pulling 12-hour swings, “consistent bedtime” isn’t realistic. Your schedule doesn’t allow it.
But your system can still be consistent. Shift work breaks the traditional advice because “bedtime” isn’t stable. So don’t anchor to bedtime. Anchor to what happens right before sleep and what happens at wake.
Your two anchors:
- Your pre-sleep runway (the last 60 minutes)
- Your wake-up routine (light, movement, caffeine after you’re up)
Pre-shift vs. post-shift routines:
- Pre-shift sleep (before nights): Treat it like “nighttime” even if the clock says 2 p.m. Dark room, low stimulation, runway first. Your wind-down might be shorter and more compressed.
- Post-shift sleep (after nights): Your body is wired. You need a stronger downshift. Reduce light exposure on the way home if possible, keep the last hour quiet, then sleep. You may need a longer decompression period.
Both versions can follow the same sequence—just adjusted for timing.
Protect your sleep window. Blackout curtains, white noise, and a “do not disturb” phone setting aren’t luxuries—they’re tools for shift workers who need to sleep when the rest of the world is awake.
If you’re in a safety-critical job, this matters even more: the goal isn’t just “fall asleep.” The goal is clear mornings (or clear wake-ups)—fewer zombie shifts, fewer near-misses, fewer “why am I so foggy?” days. For more on managing morning grogginess, we’ve written a separate guide.
“I have a crazy work schedule and no time for doctor appointments. This was the easiest thing ever—filled out some questions, got approved, and my prescription was ready pretty fast. I don’t wake up a million times a night anymore, which is honestly life-changing.” — Emily R.
Safety-First: When to Pause and Talk to a Clinician Instead of Pushing Through
Habits can support your medication. They can’t fix everything. This is the part people skip—and it’s the part that keeps you safe.
If any of the below applies to you, pause and get evaluated. Don’t “power through” with more routines or stronger sleep pressure.
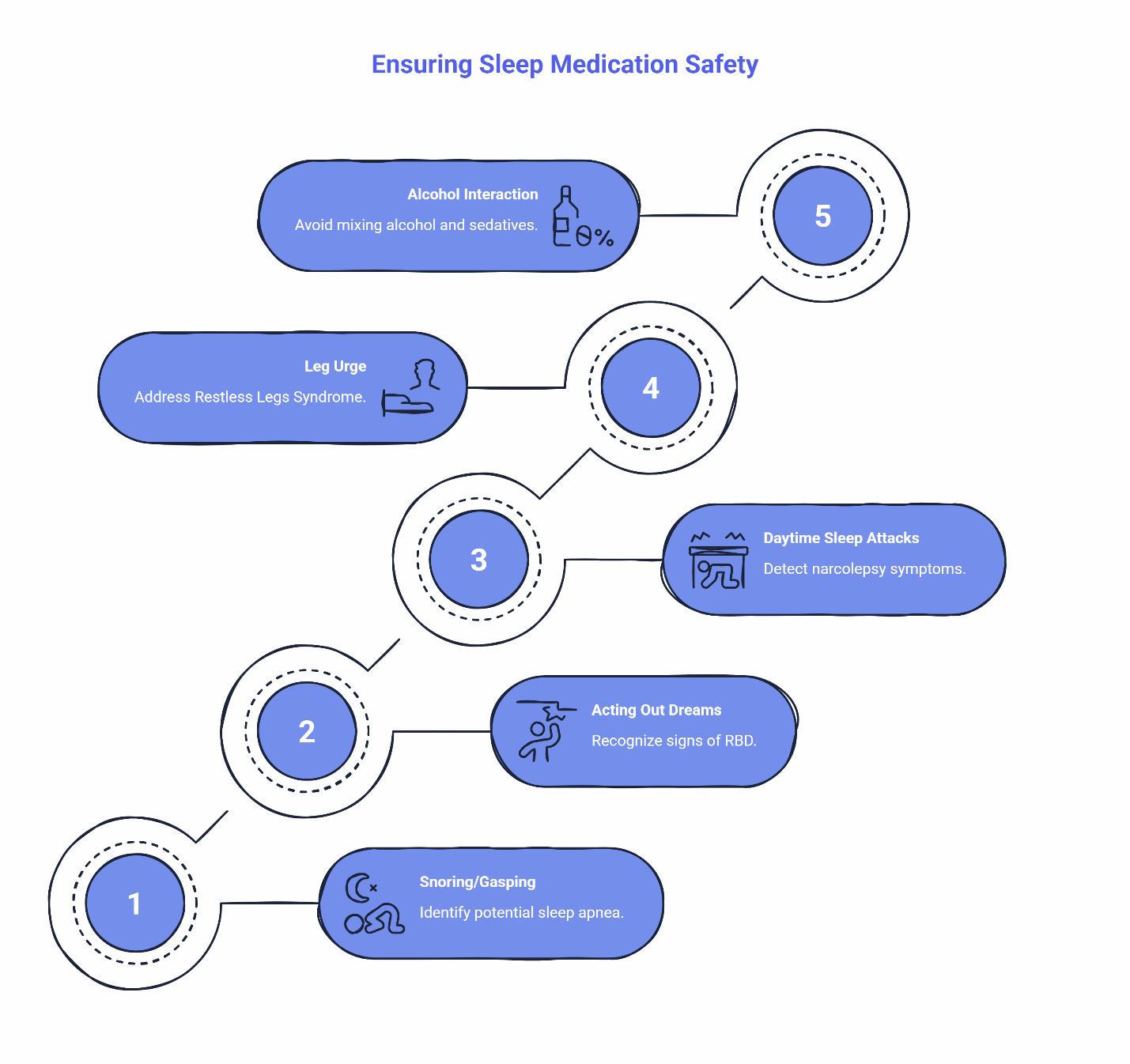
Stop and seek evaluation if you notice:
- Snoring, gasping, or breathing pauses during sleep. These may signal obstructive sleep apnea. Because certain sleep medications can affect your airway or respiratory drive, clinical guidelines generally recommend a thorough evaluation—which often includes an at-home or in-lab sleep test—to rule out obstructive sleep apnea before safely starting sedative treatments.
- Acting out dreams or violent movements during sleep. This could indicate REM Sleep Behavior Disorder (RBD). Certain common mental health and sleep medications—particularly antidepressants like SSRIs, SNRIs, and TCAs—can actually worsen or unmask RBD symptoms. However, medications like trazodone are typically considered lower risk for this specific issue. Even so, acting out dreams requires an in-person neurological evaluation, which usually involves a video sleep study to confirm the diagnosis and safely adjust your treatment plan.
- Sudden daytime sleep attacks or muscle weakness triggered by strong emotions. These are red flags for narcolepsy, which needs a full in-person sleep study to diagnose. The Narcolepsy Network Resource Center offers support for next steps.
- Uncomfortable urge to move your legs at night. Restless Legs Syndrome (RLS) can be linked to iron deficiency or other underlying conditions that need lab work and in-person evaluation, including tests for ferritin, iron, kidney function, B12, and blood sugar.
One more safety note: Alcohol and sedatives don’t mix safely. Even non-controlled sleep medications can have unpredictable interactions with alcohol. If you’re drinking regularly in the hours before bed, talk to your clinician before combining anything.
For detailed information on medication safety, see the MedlinePlus trazodone guide.
Your Habit Stacking Worksheet
Use this worksheet to pair your existing habits with one small sleep-supporting action. Prioritize consistency over exact timing.
Existing Habit (Already Happens) | Add-On Sleep Habit (Tiny) | Done |
|---|---|---|
Set my alarm for tomorrow | Switch phone to night mode | ☐ |
Brush my teeth | Dim the bathroom lights | ☐ |
Change out of work clothes | Put on sleep-only clothes (cue for brain) | ☐ |
Plug in my phone | Place phone face-down, across the room | ☐ |
Lock the door / turn off kitchen light | Start your wind-down cue | ☐ |
Take my medication | Same spot, same time relative to routine | ☐ |
7-Day Morning Clarity Tracker
Rate your morning clarity 1–10 each day. Note one thing that changed.
Day | Clarity (1–10) | What Changed? (Timing / Caffeine / Screens / Meal / Alcohol / Stress) |
|---|---|---|
1 | ||
2 | ||
3 | ||
4 | ||
5 | ||
6 | ||
7 |
After a week, look for patterns. If your clarity stays below 7, that’s useful information to bring to your clinician.
“I’ve tried a bunch of different things for my sleep, and most of them either didn’t work or made me feel like a zombie the next day. The provider actually took the time to figure out what would work best for me. Haven’t slept this well in years.” — Jessica
Next Step: Validate Your Sleep Pattern with a Quick Quiz
You’ve got the worksheet. You’ve got the habits. Now it’s worth checking whether your sleep pattern points toward something straightforward—or whether there’s a red flag worth investigating.
The Sleep Clarity Quiz takes about two minutes and helps you understand what’s actually going on—sleep onset, sleep maintenance, schedule disruption, or something else—before you commit to anything bigger.
If you want something even faster, the 6-Second Sleep Check gives you a quick gut-check on whether your sleep issues are worth addressing now.
Either way, you’re not signing up for anything. You’re just getting clearer on where you stand.
If you’re ready to explore medication options, you can review what’s available and see pricing before starting.
This article is for informational purposes only and is not medical advice. Do not start, stop, or change any medication without guidance from a licensed clinician. If you have alarming symptoms (e.g., breathing pauses, violent dream-enactment, sudden daytime sleep attacks), seek in-person medical evaluation.
Our Editorial Process:
Our expert team uses AI tools to help organize and structure our initial drafts. Every piece is then extensively rewritten, fact-checked, and enriched with first-hand insights and experiences by expert humans on our Insights Team to ensure accuracy and clarity.
About the SleepScriptMD Insights Team:
The SleepScriptMD Insights Team is our dedicated engine for synthesizing complex topics into clear, helpful guides. While our content is thoroughly reviewed for clarity and accuracy, it is for informational purposes and should not replace professional advice.