 Key Takeaways
Key Takeaways
Morning grogginess from sleep medications usually stems from timing mismatches, not wrong medications or doses—15- to 30-minute adjustments solve most clarity issues.
- Timing Beats Dosing: Shifting your medication window by 15 to 30 minutes typically eliminates morning fog without changing medications or increasing doses.
- Universal 30-60 Minute Rule: All three medications—Hydroxyzine, Trazodone, and Clonidine—work best when taken 30 to 60 minutes before lights-out to align peak sedation with sleep onset.
- Clarity Scoring Guides Adjustments: Rating morning alertness on a 1-10 scale for seven nights reveals whether to shift earlier (persistent fog) or later (early waking).
- Three Disruptors Undermine Results: Alcohol fragments sleep architecture, caffeine disrupts sleep for 8-12 hours, and blue-light screens suppress melatonin—avoid all three near dose time.
- Consistency Outperforms Precision: Taking medication at the same pre-bed cue nightly produces better outcomes than trying to find the perfect minute.
First-week timing adjustments typically deliver clear mornings without medication changes.
Adults managing insomnia through telehealth will gain immediate, actionable strategies for optimizing non-controlled sleep medications, preparing them for the detailed timing protocols and safety guidelines that follow.
~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~
The alarm goes off. Your head feels heavy. The brain fog from last night’s sleep medication hasn’t lifted, and you have a meeting in an hour. You took the pill at the right time… didn’t you?
Maybe I should have taken it earlier. Or was it too early last time?
You’re not alone in this confusion. The cycle of second-guessing your dose window, waking up groggy, and wondering whether to adjust your medication is exhausting. But here’s what most people don’t realize: you probably don’t need a different medication or a higher dose.
The difference between waking up clear-headed and struggling through morning fog often comes down to a 15- to 30-minute adjustment in when you take your medication—not which medication you take or how much. Most patients who report grogginess aren’t experiencing a medication problem; they’re experiencing a timing mismatch between their dose window and their natural sleep-wake cycle.
Quick Answer: Your Timing Window Cheat Sheet
Here’s the practical framework you need. This table shows you where to start based on your target bedtime, what to expect, and how to adjust if your morning clarity drops below 7 out of 10.
Target Bedtime | Hydroxyzine | Trazodone | Clonidine | Expected AM Feel | If Clarity <7… |
|---|---|---|---|---|---|
9:30 PM | Take at 9:00 PM | Take at 9:00 PM | Take at 9:00 PM | Sedative effects typically fade by 6:00 AM with 7-8h sleep | Residual fog? Shift 15-30 min earlier. Early wake? Shift 15-30 min later. |
10:30 PM | Take at 10:00 PM | Take at 10:00 PM | Take at 10:00 PM | Sedative effects typically fade by 7:00 AM with 7-8h sleep | Same adjustment logic |
11:30 PM | Take at 11:00 PM | Take at 11:00 PM | Take at 11:00 PM | Sedative effects typically fade by 8:00 AM with 7-8h sleep | Same adjustment logic |
12:30 AM | Take at 12:00 AM | Take at 12:00 AM | Take at 12:00 AM | Sedative effects typically fade by 9:00 AM with 7-8h sleep | Same adjustment logic |
Key timing principles: All three medications work best when taken 30 to 60 minutes before you turn off the lights. This gives each medication time to reach peak effectiveness as you’re falling asleep. All timing windows assume physician-approved use and should be individualized with your provider.
Important safety note: While sedative effects typically fade after 7-8 hours of sleep, these medications remain in your system longer. Use caution with driving or operating machinery during your first few mornings until you know how your body metabolizes the medication.
Pick the Right Key for Your Lock (Onset vs. Maintenance)
Not all sleep medications work the same way, which is why timing matters so much. Think of it like choosing the right key for your lock—the medication has to match your specific sleep problem.
These non-addictive sleep medications are effective, safe, and widely used as first-line options for insomnia. The key is matching the right medication to your specific sleep pattern.
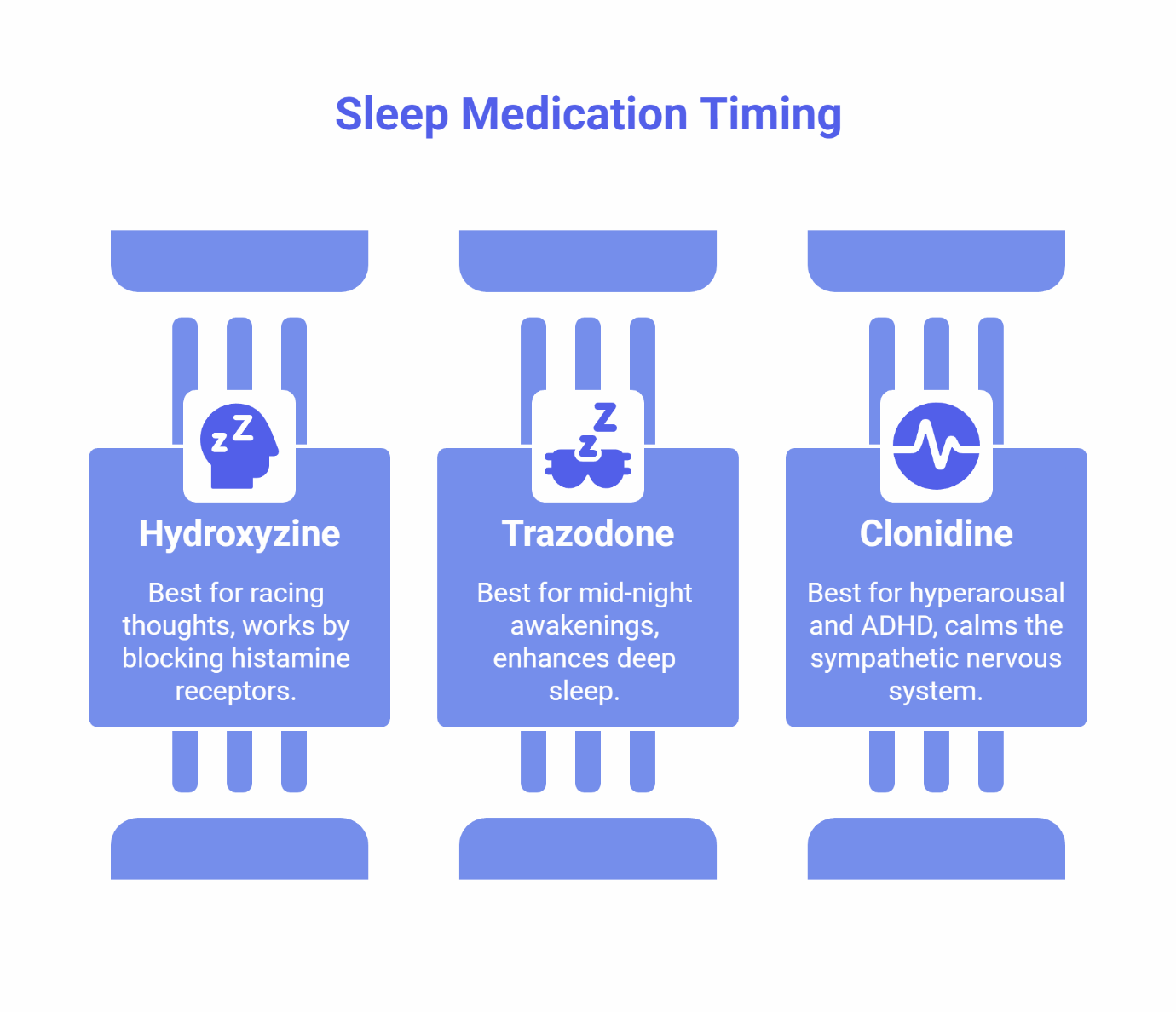
Hydroxyzine: Best for Racing Thoughts
Hydroxyzine is your go-to when the problem is falling asleep because your mind won’t shut off. It works by blocking histamine receptors, which reduces mental arousal and creates a calming effect.
Timing window: 30 to 60 minutes before you turn off the lights. This gives the medication time to reach peak effectiveness right when your head hits the pillow.
What to expect: Most people report a quieter mind and smoother sleep onset. The primary sedative effect typically lasts 4 to 6 hours, though the medication remains in your system longer. Most patients wake up clear-headed, but caution is advised during the first few mornings until you know how you metabolize the medication.
Learn more about Hydroxyzine →
Trazodone: Best for Mid-Night Awakenings
Trazodone is the better choice when you can fall asleep just fine, but you wake up at 2:00 or 3:00 AM and struggle to get back to sleep. It enhances deep, slow-wave sleep—the most restorative sleep stage.
Timing window: 30 to 60 minutes before you turn off the lights. Trazodone takes time to reach peak levels, so timing it before bed helps transition you smoothly into sleep and maintains deep sleep through the night.
What to expect: Fewer interruptions and deeper sleep. Some patients—clinical studies suggest 20 to 40 percent—report mild morning grogginess, which is usually resolved by shifting the dose window 15 to 30 minutes earlier.
Clonidine: Best for Hyperarousal and ADHD
Clonidine works differently—it calms your sympathetic nervous system, which is the body’s “fight or flight” response. This makes it especially effective if you feel wired but tired, or if you have ADHD-related sleep disturbances.
Timing window: 30 to 60 minutes before lights-out, similar to Hydroxyzine and Trazodone.
What to expect: A calmer body and reduced physical restlessness. Most people report low hangover risk because Clonidine’s sedative effects clear smoothly overnight.
The First-Week Timing Loop (4 Steps)
Your first seven nights on a new sleep medication aren’t about finding the perfect dose—they’re about finding your perfect timing window. Here’s the simple system that works.
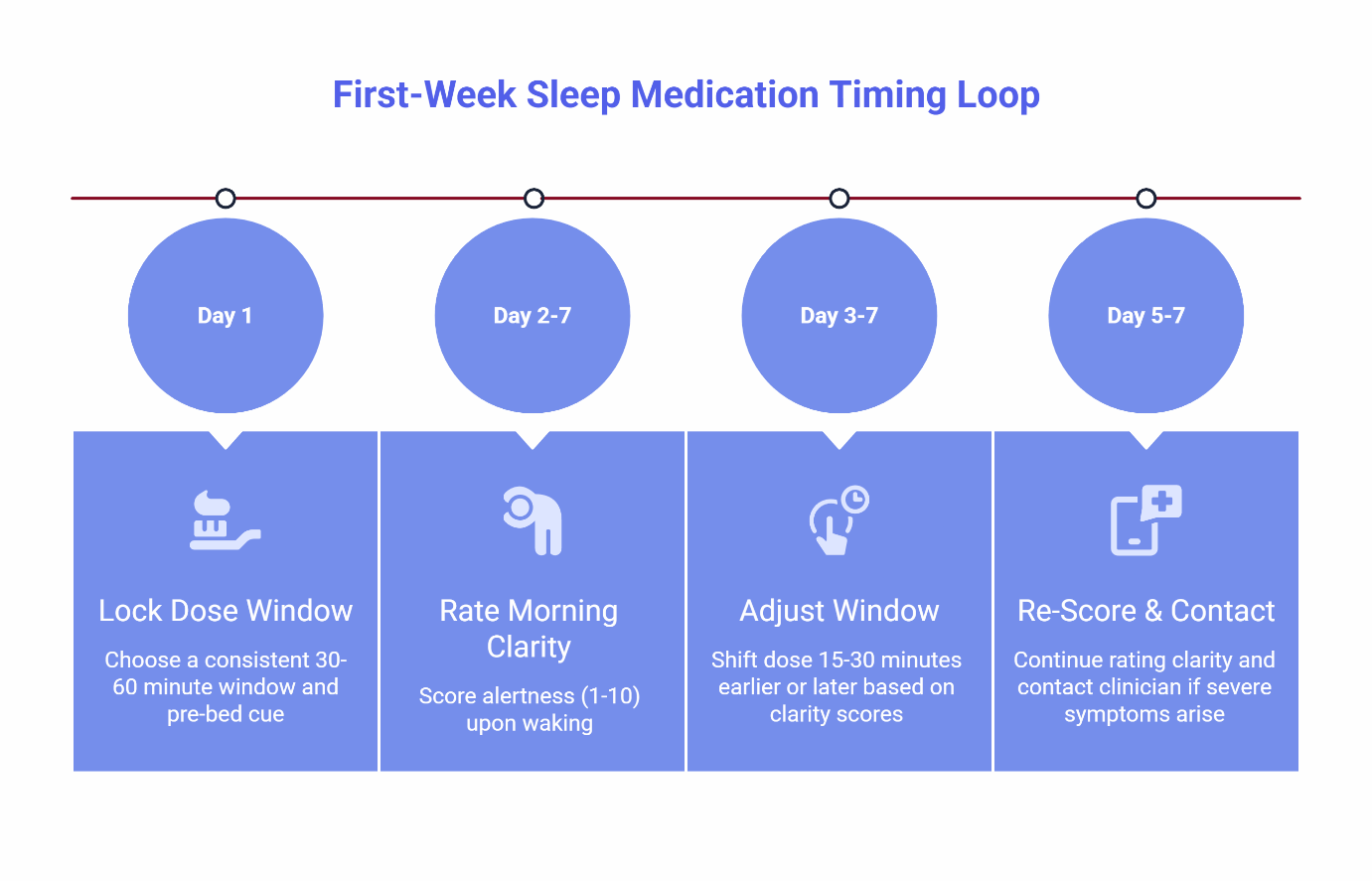
Step 1: Lock a 30- to 60-Minute Dose Window
Pick a consistent time to take your medication and tie it to a pre-bed cue you already do every night. This could be brushing your teeth, setting your phone alarm, or turning on your bedroom air filter.
The key is consistency. Taking your medication at 10:30 PM one night and 11:15 PM the next creates unpredictable results.
Step 2: Rate Your Morning Clarity (1 to 10 Scale)
When you wake up, give yourself a clarity score. A 7 or higher means you feel alert, focused, and ready to start your day without needing an extra hour to “shake off” the medication. A score below 7 means you’re experiencing residual sedation—that brain fog or heaviness that lingers past your first cup of coffee.
Step 3: Adjust Your Window Based on Two Patterns
If your clarity score stays below 7 for two or more consecutive days, make one of these adjustments:
- Residual drowsiness lasting past 10:00 AM? Shift your dose window 15 to 30 minutes earlier. This gives your body more time to metabolize the medication before you need to be fully functional.
- Waking up too early (before your alarm)? Shift your dose window 15 to 30 minutes later. This ensures the medication’s effects last through your target wake time.
Step 4: Re-Score and Contact Your Clinician if Needed
After making an adjustment, continue rating your morning clarity for another two to three days. Most people find their ideal window within five to seven nights. If you experience severe grogginess, dizziness, or any concerning new symptoms, message your clinician before your next dose.
What to Avoid Near Dose (Protect Morning Clarity)
Even a perfectly timed dose can be undermined by what you do in the hours leading up to it. These three factors consistently worsen morning clarity and should be avoided on nights you take your medication.
Alcohol Should Be Avoided
Combining alcohol with sleep medications should be avoided. Alcohol disrupts your sleep architecture, causing fragmented, lower-quality sleep even if you’re technically unconscious for eight hours. Clinical data indicates that alcohol significantly reduces sleep quality and increases nighttime awakenings, which means you’ll wake up feeling unrested even if your medication helped you fall asleep.
The practical rule: skip alcohol on nights you take your sleep medication.
Caffeine Cutoff Matters More Than You Think
The standard advice to “avoid caffeine after 2:00 PM” isn’t precise enough. Caffeine’s disruptive effects on sleep quality can persist for 8 to 12 hours depending on the dose and your individual metabolism.
A controlled trial published in the journal Sleep found that high caffeine doses can disrupt sleep even when consumed many hours before bedtime. A meta-analysis modeling caffeine clearance suggests cutoffs can extend to 9 to 10 hours for coffee, and longer for higher-dose products—though individual sensitivity varies considerably.
The practical rule: if you’re taking your medication at 10:30 PM, your last caffeinated beverage should be no later than 2:30 PM—and earlier if you’re sensitive to caffeine or consuming high doses (200+ mg). Plan a cutoff of at least 6 hours, and often 8-12 hours depending on dose and sensitivity.
Blue-Light Screens Suppress Melatonin
Your phone, tablet, and laptop emit blue wavelengths of light that signal to your brain that it’s still daytime. This suppresses melatonin production, making it harder for your medication to work effectively. Exposure to blue light (460-480nm) at night directly suppresses melatonin and disrupts your natural sleep-wake cycle.
The practical rule: screens off 30 to 60 minutes before you take your medication. If you absolutely need to use a device, enable night mode or use blue-light-blocking glasses.
Travel & DST: Shift Without Ruining Tomorrow
Business trips and Daylight Saving Time create predictable timing challenges. The key is shifting your dose window gradually toward your destination schedule rather than trying to jump directly to the new time zone.
The 30- to 60-Minute Pre-Shift Rule
Starting two to three nights before travel, shift your dose window 30 to 60 minutes closer to your destination bedtime each night. If you’re traveling from New York to Los Angeles (a 3-hour difference), you’d shift your dose from 10:30 PM to 11:00 PM on night one, 11:30 PM on night two, and 12:00 AM on night three. By the time you land, your body is already partially adjusted.
Standard travel health protocols recommend gradually adjusting sleep schedules before departure to minimize jet lag, and this principle applies equally to medication timing.
Anchor to Destination Clock, Not Home Clock
Once you arrive, take your medication based on the local bedtime—not when your body thinks it should be sleeping. This helps your circadian rhythm align faster with the new time zone.
Understanding “Social Jet Lag”
For Daylight Saving Time transitions, sleep specialists emphasize that even a one-hour clock change can create what’s known as “social jet lag.” This misalignment explains why circadian-aligned routines help reduce the impact. Using the same gradual-shift approach—moving your timing window 30 minutes earlier or later across two nights—minimizes disruption to both your sleep and morning clarity.
Support Your Adjustment
Your body is already working harder to adjust during travel. Avoiding alcohol and limiting late caffeine can help you maintain better morning clarity during the transition.
Before You Start: Eligibility & Safety
These medications are safe and effective for the right patients. Here’s what you need to know before beginning.
You may be eligible if you:
- Are between 18 and 65 years old
- Are not pregnant and not planning to become pregnant
- Have no major medical, mental health, or substance use conditions that could make sleep medications unsafe
- Are not currently taking benzodiazepines or other controlled sleep medications
Snoring or gasping during sleep? You’ll need to complete an at-home sleep test before treatment begins. Most patients start testing within a few days.
We cannot treat certain conditions online: If you experience symptoms of narcolepsy (sudden daytime sleep attacks), REM Sleep Behavior Disorder (acting out dreams physically), or Restless Legs Syndrome, we’ll refer you to a local specialist for in-person evaluation.
Not sure if you qualify? Take the 6-Second Sleep Check or try the Sleep Clarity Quiz to learn more about your sleep pattern.
How SleepScriptMD Works
SleepScriptMD offers two convenient approaches to help you find your ideal timing window.
AI-Assisted Asynchronous Care (Where Available)
Complete an online assessment at your convenience. Our AI-assisted system evaluates your responses in real-time, with 95% of patients receiving treatment recommendations and prescriptions within minutes. If additional clarification is needed, we’ll contact you via text or recommend a brief virtual session.
Cost: $45 per month or $120 for 90 days. Medication cost at your pharmacy is separate and often covered by insurance.
Virtual Telehealth Session (Some States)
Schedule a live video session with one of our expert practitioners for a personalized evaluation and treatment plan. Appointments are often available within five days.
Cost: $110 for a 25-minute intake session (includes your first month of service and a 30-day medication supply if prescribed). Follow-ups are $85 for 15 minutes.
See Pricing & State Requirements →
Compare Our Treatment Options →
Frequently Asked Questions
What if I still feel groggy after adjusting my timing?
Keep the same dose and shift your window earlier by 15 to 30 minutes for two nights, then re-score your morning clarity. If you’re still below 7 after this adjustment, message your clinician. The issue may not be timing—it could be medication fit.
What if I have an early meeting the next day?
Move your timing window 15 to 30 minutes earlier the night before to give your body extra time to metabolize the medication. Also avoid alcohol and caffeine after 2:00 PM, and implement a strict device curfew 30 to 60 minutes before your dose.
What if I snore or have been told I stop breathing during sleep?
You’ll need to complete an at-home sleep test before any sleep medication can be prescribed. Prescriptions are only issued after your test results are reviewed. Most patients begin testing within a few days of starting the intake process.
Can I take my medication at different times on weekends?
Consistency produces better results. Your body’s sleep-wake cycle responds best to predictable timing. If you need to shift your schedule on weekends, keep the variation to 30 minutes or less and use the same adjustment principles—shift gradually rather than jumping two hours forward or backward.
How long will it take to find my ideal window?
Most people find their ideal timing window within five to seven nights using the clarity-score feedback loop. The key is making small adjustments (15 to 30 minutes) rather than large jumps, and giving each adjustment two to three nights before evaluating results.
Which medication should I choose?
The best medication depends on your specific sleep pattern. See which medications we offer or compare Trazodone, Hydroxyzine, and Clonidine to find the right fit.
Ready to stop guessing and start sleeping?
Disclaimer: This content is for educational purposes only and is not a substitute for medical advice. Prescriptions are issued after physician review per state telehealth rules. Always consult your healthcare provider before starting or adjusting any medication.
By: SleepScriptMD Insights Team
Reviewed by: Dr. David Danish, MD (Chief Psychiatric Officer) and Dr. Peter Kelly, DO (Chief Medical Officer)